Senescent alopecia
Senescent alopecia
Clinical features Senescent (senile, involutional) alopecia most probably represents a physiological event, as the majority of elderly people develop loss of hair pigment (canities), and there is a diffuse decrease in the density and thickness of the hair in the scalp, axillary, and pubic regions (Fig. 22.89).1–3 Typically, patients with senile alopecia are older than 50, although the predictive value of age in total hair count has been found to be limited.4 Patients have no relevant family history of alopecia. In some animal models, such as female squirrel monkeys (Saimiri boliviensis), age-related alopecia has been observed.5
Differential diagnosis The differential diagnosis is mainly with those alopecias that show a bandlike pattern of hair loss, such as alopecia areata in an ofiasic pattern and frontal fibrosing alopecia especially when the clinical history is not very clear (Fig. 22.51). Nevertheless, the clinical findings of preservation of ostium follicles and histologic findings of a peribulbar inflammatory cell infiltrate are enough to allow the diagnosis of alopecia areata to be made. In fibrosing frontal alopecia, there is clinical evidence of erythema and perifollicular scaling and histologic features of an interphase lymphocytic inflammatory cell infiltrate in the upper segment.13–15
Late traction alopecia is often indistinguishable on histology grounds from end-stage cicatricial alopecia. In difficult cases, clinicopathological correlation is essential.10,13
The hair-pull/hair-pluck tests are normal with no increase in the number of telogen hairs.
Histologic features Senescent alopecia is a controversial concept. It has characteristics that defined it as an entity and probably related to accumulative oxidative stress directly related to age; yet, sometimes the separation from androgenic alopecia or telogen effluvium is not clear.6–9
Horizontal sections are very useful in the diagnosis of senile alopecia, particularly if the biopsies are from two different sites, because they allow a comparative evaluation in relation to the diffuse or localized nature of the process allowing distinction from other types of alopecia.1
1082 Diseases of the hair
Histologically, there is a slight decrease in the number of follicular units and terminal hair follicles, with a normal ratio between terminal and vellus hair follicles and between anagen and telogen hair follicles (Fig. 22.90).
Differential diagnosis Distinction from telogen effluvium and from androgenetic alopecia may be difficult but the pattern of diffuse involvement, without an increase in the percentage of telogen hairs or an increase in the number of vellus hairs, is very suggestive of senile alopecia.10
Fig. 22.51 Traction alopecia, ophiasis and frontal fibrosing alopecia pattern of hair loss. The patient on the left with the ophiasis pattern also has a superimposed tinea. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.

Fig. 22.87 Fringe sign: note the retained hairs along the frontal and temporal rim. Courtesy of J. Cadavid, MD, Clínica Medellín, Medellín, Colombia.
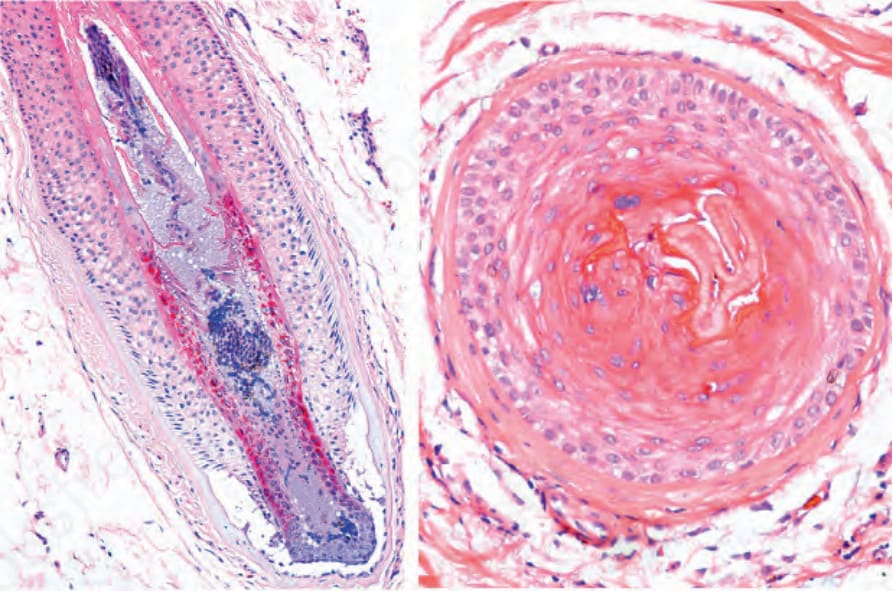
Fig. 22.88 Traction alopecia, early stage: vertical and horizontal sections of a hair follicle showing marked damage to the inner root sheath.

Fig. 22.89 Senescent alopecia: the reduction in the hair density is evident in the lighter areas of the scalp.
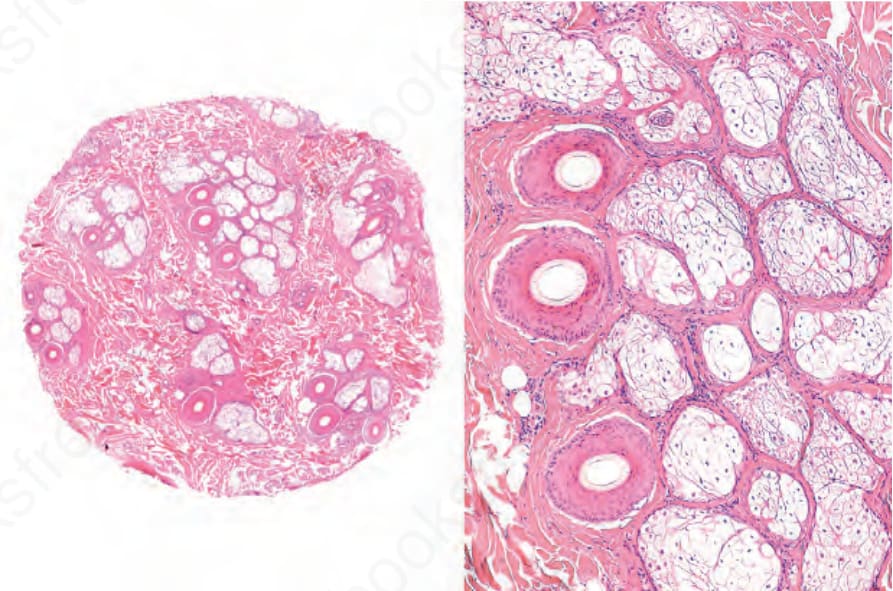
Fig. 22.90 Senile alopecia: there is a subtle decrease in the number of hair follicles and follicular units with preservation of the ratios between the number of terminal and vellus hair follicles and the hair follicles in anagen and telogen. There is an apparent increase in the amount of connective tissue between the follicular units which should not be confused with a scarring alopecia.