Pressure alopecia
Pressure alopecia
Clinical features Abel and Lewis first described postoperative (supine or pressure) alopecia in 1960.1 Pressure alopecia is an uncommon complication of surgery and is reported mainly in adults who undergo anesthesia, typically affecting the occiput and resulting from head immobilization during prolonged periods of unconsciousness. The pressure induces tissue hypoxia and ischemia. Most alopecia is temporary, but rare cases are permanent. Pressure alopecia was first described after long-lasting gynecological operations.1 It has also been reported after cardiac, gynecological, abdominal, esthetic, and breast reconstruction surgery. Further associations include numerous surgical and therapeutic procedures, and occurrence in severely ill or comatose patients.2–6 It is more frequent after cardiovascular surgery, prolonged endotracheal intubation, prolonged head immobilization, and the intraoperative use of the Trendelenburg position.7–10
Patients with this condition typically complain of occipitoparietal pain and tenderness within 24 hours of surgery. Hair loss is usually complete within 3–28 days after surgery. Most cases are self-limiting with regrowth occurring within 12 weeks. However, there are reported cases of permanent alopecia.11
Histologic features The histopathology in early stages shows vascular thrombosis and necrosis of the dermis and subcutaneous tissue. Later, the microscopic findings include features in common with trichotillomania, including the presence of pigment casts, abundant catagen and telogen follicles, melanophages, and apoptotic bodies.12–14
Differential diagnosis Distinction from other causes of localized hair loss is usually easy and can be done on clinical grounds alone. However, the differential diagnosis with chronic radiodermatitis after intraoperative fluoroscopic imaging may be problematic. In these cases, the antecedent of having been exposed to radiation and the location of the bald patches along the scalp margins with an ophiasis pattern is an important clue. The latter pattern occurs because this is the area of the scalp that receives the highest dose of radiation during fluoroscopy.15,16
1081 Nonscarring alopecias
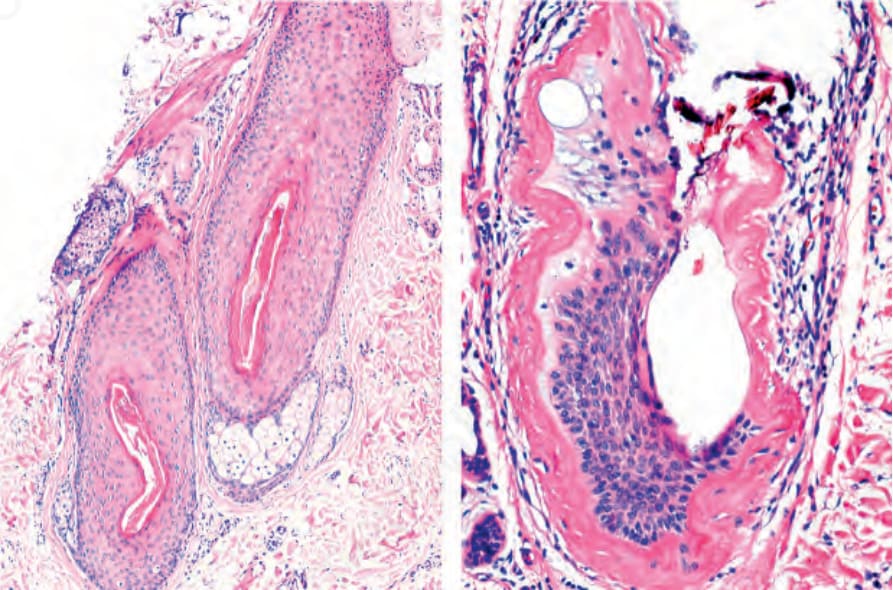
Fig. 22.84 Trichomalacia: left panel, note a hair follicle showing irregularities in the thickness of its wall. Right panel, this hair follicle has almost lost all its structural integrity. Courtesy of the L.E. Muñoz, Cali, Colombia.