Psoriatic alopecia
Psoriatic alopecia
Clinical features Psoriatic alopecia was first described in 1972 by Shuster.1 Between 50% and 80% of patients with psoriasis will develop scalp involvement at different stages during the course of the disease.2,3 Psoriatic alopecia may be caused by psoriasis itself, by systemic or topical therapy, or may be associated with other autoimmune diseases particularly alopecia areata.4 The most common form of presentation is involvement of skin already affected by psoriasis (Fig. 22.72). Another way in which psoriasis may cause hair loss is through effluvium telogen particularly in the course of erythrodermic or generalized pustular psoriasis.5
The majority of the patients with psoriatic alopecia present with a reversible nonscarring alopecia. Only a small percentage of patients will develop scarring alopecia secondary to psoriasis. This seems to be related to the duration and intensity of the inflammatory process.6–8 However, it is not always clear which patients will develop a reversible nonscarring alopecia or scarring alopecia.3
Differential diagnosis The most important histologic differential diagnosis is with alopecia areata. In alopecia areata, there are no epidermal changes of psoriasis and there is no loss of sebaceous glands.
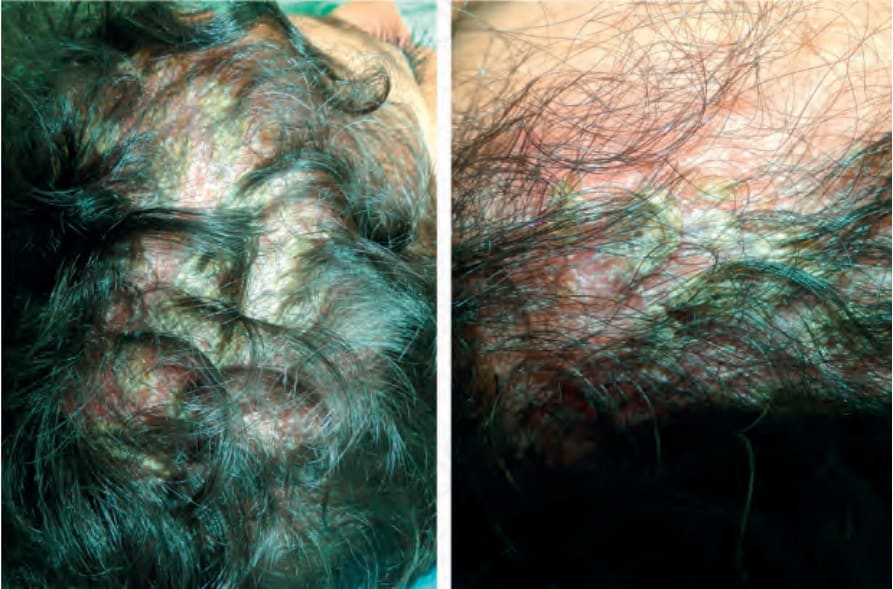
Fig. 22.72 Psoriasis. Note a thick scale covering an area of alopecia simulating tinea capitis. Courtesy of C. Velázquez, MD, CES, Medellín, Colombia.