Postinflammatory hyperpigmentation
Postinflammatory hyperpigmentation
Clinical features Postinflammatory hyperpigmentation is relatively common and may occur following almost any inflammatory dermatosis and after the application of exogenous substances (Figs 20.46 and 20.47).1,2 Hyperpigmentation is also commonly seen after trauma to the skin and may occur following cosmetic
1013 Riehl melanosis
procedures such as chemical peeling. The changes are seen in all races but are more common and noticeable in people with dark skin.1,2 Dermatoses such as lichen planus, lichenoid drug eruptions, fixed drug eruptions, and lupus erythematosus (where there is usually prominent damage of basal cells) are more often associated with pigmentary changes. Hypo- and hyperpigmentation not uncommonly occur in the same patient. Hyperpigmentation of some areas of the skin, for example the periorbital area, is more common than involvement of other parts of the skin and multiple exogenous and endogenous etiologies have been associated with it.3 In some instances, patients present with established hyperpigmentation and cannot recall an episode of skin inflammation. Spontaneous resolution of the pigmentation is usually partial at best and treatment is frequently disappointing.
with geographic borders and occasional focal hypopigmented macules on the dorsum of the forearms.1 Most cases are bilateral and there is predilection for postmenopausal females. Very rare cases may occur in males.2
Pathogenesis and histologic features The changes do not appear to be associated with estrogens, pregnancy, or hormone replacement therapy and although the initial report found no clear relationship with sun exposure, it has recently been proposed that it may be associated with chronic sun damage.1–3 An association with hypertension and/or antihypertensive drugs has been suggested.1
Pathogenesis and histologic features The pathogenesis of postinflammatory hyperpigmentation may be explained by the damage to keratinocytes and melanocytes with resulting pigment incontinence and phagocytosis of the melanin by macrophages (melanophages) (Fig. 20.48). In vitro studies have demonstrated that normal human epidermal melanocytes become swollen and more dendritic with an increase in the amount of immunoreactive tyrosinase when they are cultured for several days with arachidonic acid metabolites, including prostaglandin D2, leukotriene B4, C4, D4, thromboxane B2, and eicosatetraenoic acid.4–8 The effect of leukotriene C4 appears to be particularly intense. These findings suggest an important role of melanocytes in the induction of postinflammatory hyperpigmentation. A further proposal suggests that fibroblast-derived growth factors, particularly keratinocyte growth factor, on its own or in association with interleukin-1alpha, may play a role in inducing the hyperpigmentation.9
Histologically, epidermal atrophy, basal hyperpigmentation, elastosis, and telangiectasia are described.

Fig. 20.46 Postinflammatory hyperpigmentation: prominent hyperpigmentation after the application of henna for cosmetic purposes. By courtesy of the Institute of Dermatology, London, UK.
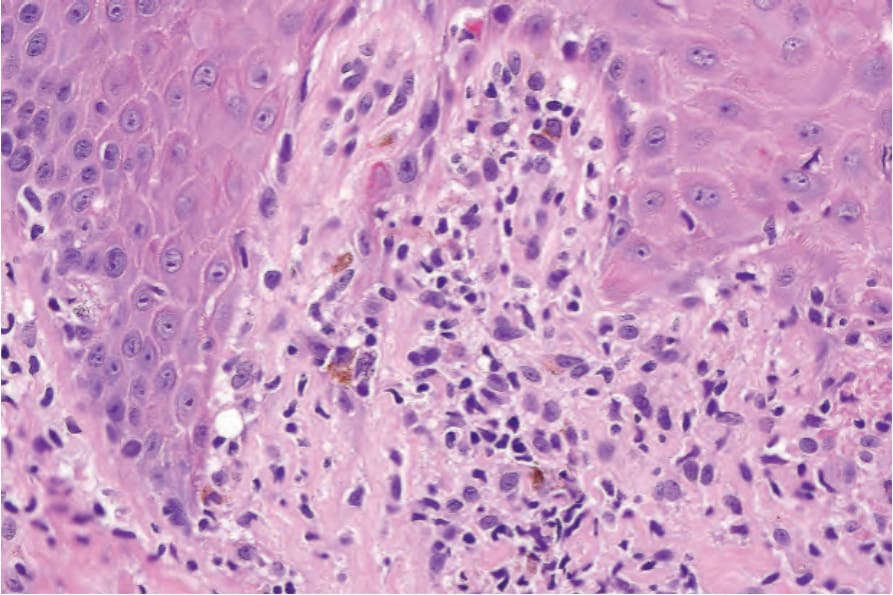
Fig. 20.48 Postinflammatory hyperpigmentation: focal pigment incontinence in a case of lichen planus.
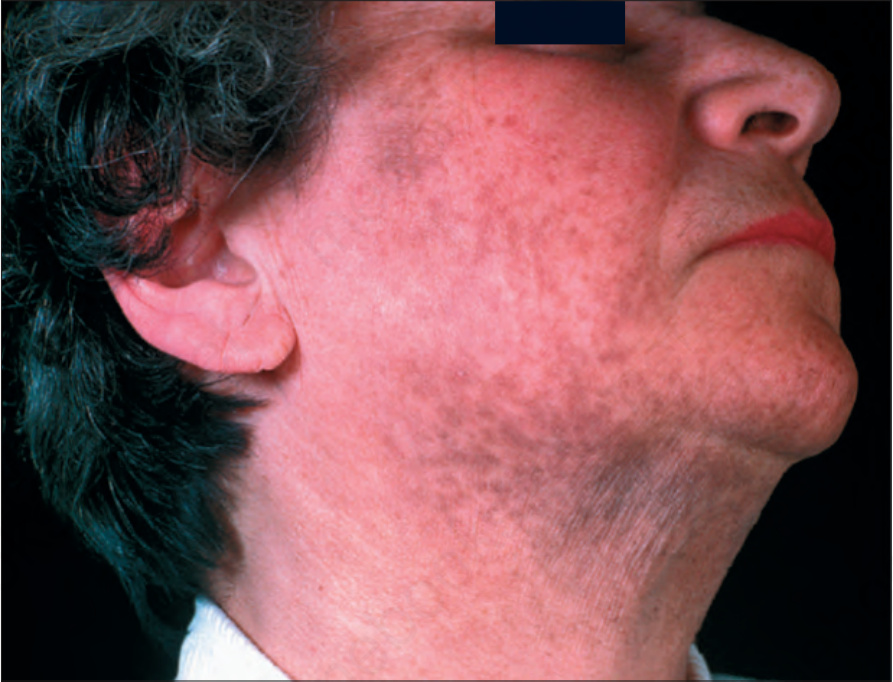
Fig. 20.49 Riehl melanosis: prominent patchy hyperpigmentation of the face. By courtesy of the Institute of Dermatology, London, UK.