LEOPARD syndrome
LEOPARD syndrome
representing entrapped follicular structures with cystic change or focal basaloid buds – is often seen (see Fig. 20.41).27
Clinical features LEOPARD syndrome is a rare congenital syndrome inherited in an autosomal dominant manner with variable expression. It is characterized by lentiginosis, electrocardiographic conduction abnormalities (due to hypertrophic cardiomyopathy), ocular hypertelorism, pulmonary valve stenosis, abnormalities of the genitalia (particularly cryptorchidism and hypospadias), growth retardation (in up to 50% of individuals), and sensorineural deafness (Fig. 20.45).1–6 Lentigines may rarely be absent. When present, they appear after the first 4 or 5 years of life and by adolescence patients have perhaps developed hundreds of lesions.7 Lentigines have a predilection for the upper trunk and neck but can occur anywhere in the skin (including genitalia, palms, and soles) and sclera sparing other mucosal surfaces. Additional findings include mild mental retardation, involvement of aortic and mitral valves, focal hypopigmentation, axillary freckling, café-au-lait spots (in up to 80% of patients and usually preceding the lentigines), interdigital webs, onychodystrophy, dermatoglyphics, hyperelasticity of the skin, and steatocystoma multiplex.3,4–12 Corneal choristomas, granular cell tumors, morphea, and acro-osteolysis have also been documented.5,12,13 Rare associations include Werner syndrome and Chiari malformation.14,15 Occasional associations with hematological malignancies and multiple granular cell tumors have been reported.16–18 It has been demonstrated that LEOPARD syndrome and Noonan syndrome (facial dysmorphology, congenital cardiac defects, and short stature) are allelic disorders.19,20 Generalized lentiginosis has been documented in patients with no other evidence of LEOPARD syndrome and it is not clear whether these patients are part of the spectrum of the disease.21 Males appear to be more affected than females.
The lentigines show histologic features indistinguishable from ordinary lentigines.
Epithelioid blue nevi (pigmented epithelioid melanocytomas) are located in the dermis, lack a junctional component, and are composed of epithelioid, polygonal pigmented melanocytes interspersed with short spindled pigmented melanocytes (Fig. 20.43). Melanophages are seen throughout the tumor.17 Cytological atypia is mild and mitotic figures are rare. These tumors are identical to those occurring in a sporadic setting. As mentioned before, these proliferations have been classified within the spectrum of the so-called pigmented epithelioid melanocytoma, a term that includes pigment synthetizing melanoma (animal-type melanoma), a lesion that occurs sporadically and is regarded as of low-grade malignant potential.34 Loss of expression of protein kinase A regulatory subunit type alpha and recurrent alterations in PRKAR1A and PRKCA genes have been found in some of these lesions but not in other melanocytic tumors.50,51
Pathogenesis and histologic features Mutations in the PTPN11 (tyrosine phosphatase SHP2) gene located on chromosome 12q24 have been found in up to 90% of patients with
1012 Disorders of pigmentation
A
B
LEOPARD syndrome,20–22 the same gene identified in patients with Noonan syndrome. However, in LEOPARD syndrome different mutations (the most common being T468M and Y279C mutations) have been found in the PTPN11 gene.22–24 PTPN11 is the gene encoding the nonreceptor-type protein phosphatase SHP-2. It has been suggested that some PTPN11 mutations are associated with typical Noonan syndrome and other mutations, including the Y279C mutation, are associated with a Noonan syndrome phenotype plus multiple lentigines and café-au-lait spots.22 This group of autosomal dominant syndromes are now referred to as RASopathies as they are caused by germline mutations in the RAS/RAF/MEK/ERK mitogen-activated protein kinases (MAPKs) pathway.25 PTPN11 mutations can cause epidermal growth factor-induced phosphoinositide 3-kinase/AKT/ glycogen synthase kinase 3beta signaling which may be of importance in the pathogenesis of the syndrome.26 Missense mutations in the RAF1 gene have been found in patients with no PTPN11 mutations.27 RAF1 gene encodes a serine-threonine kinase that activates MEK1 and MEK2 (mitogen-activated protein kinases). This mutation is particularly associated with hypertrophic
cardiomyopathy. In a few cases, no mutations of PTPN11 or RAF1 are present. BRAF mutations have also rarely been described.28
The lentigines and café-au-lait spots in LEOPARD syndrome are identical histologically to ordinary lentigines and café-au-lait spots. Giant melanosomes are seen in keratinocytes and melanocytes in lesional skin.29 It has been proposed that the lentigines are caused by increased melanin production induced by the SPH2 mutations with contribution by activation of AKT/mTOR signaling.29
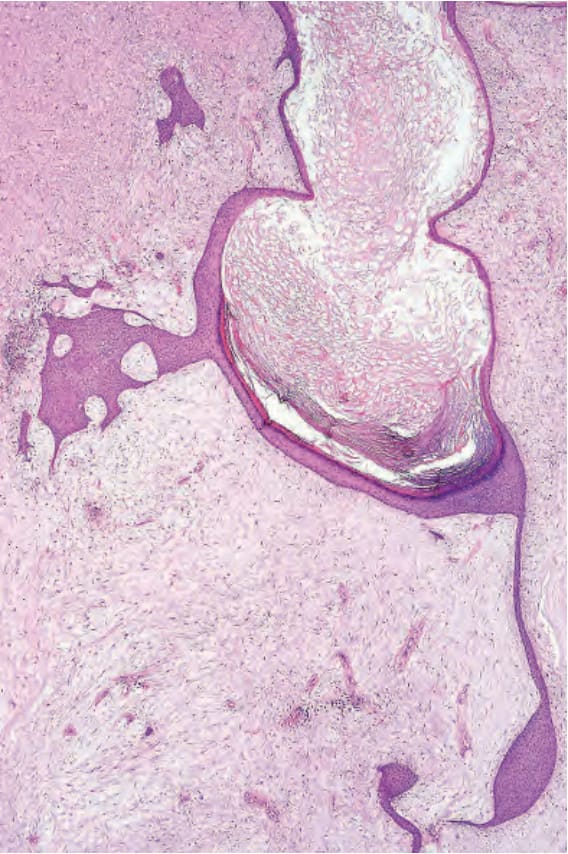
Fig. 20.41 Cutaneous angiomyxoma: dermal poorly cellular angiomyxoma with cystically dilated follicular structure.
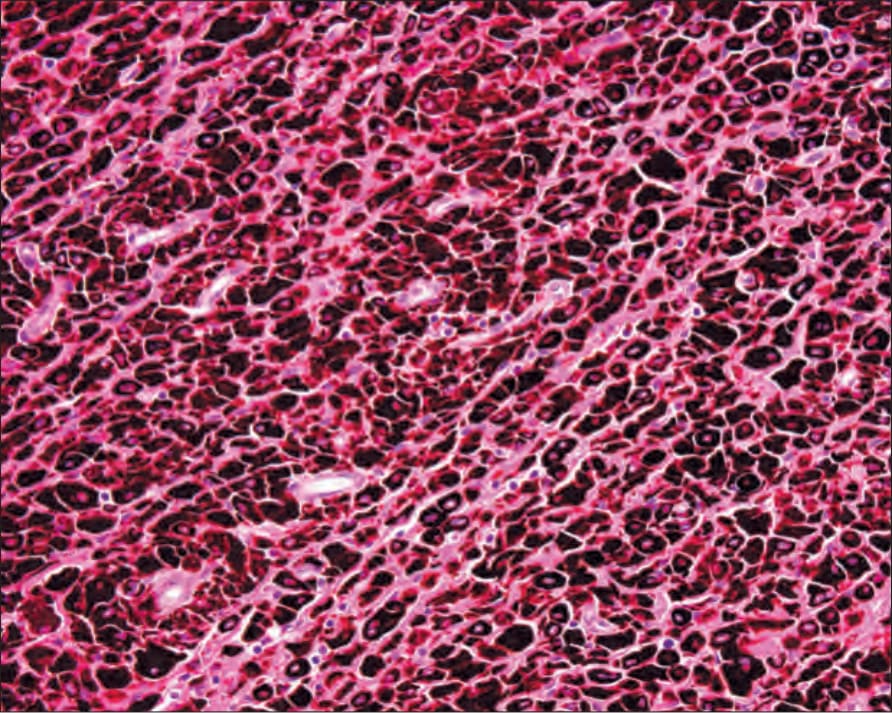
Fig. 20.43 Epithelioid blue nevus (pigmented epithelioid melanocytoma): deeply pigmented epithelioid melanocytes.

Fig. 20.45 LEOPARD syndrome: prominent lentigines on (A) the dorsum and (B) the palms of the hands. By courtesy of the Institute of Dermatology, London, UK.

Fig. 20.46 Postinflammatory hyperpigmentation: prominent hyperpigmentation after the application of henna for cosmetic purposes. By courtesy of the Institute of Dermatology, London, UK.
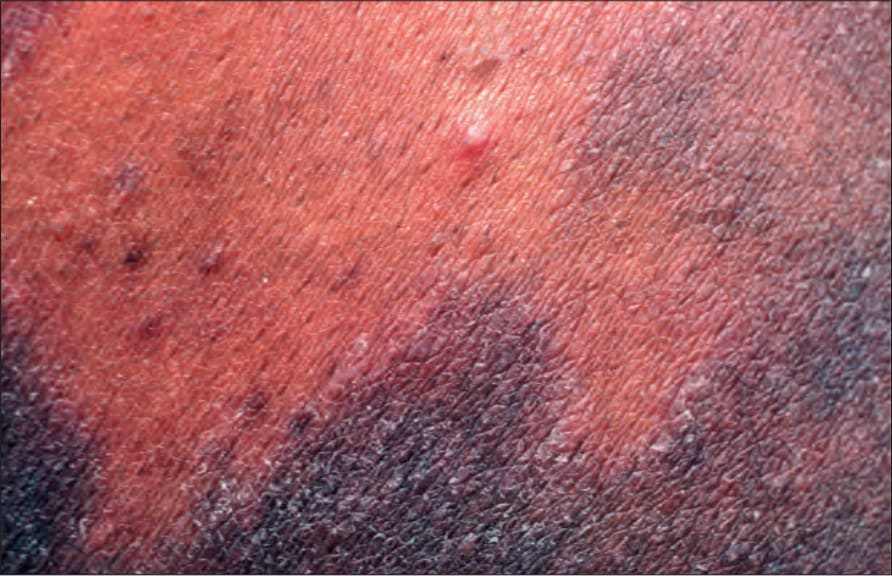
Fig. 20.47 Postinflammatory hyperpigmentation: marked hyperpigmentation after resolution of lichen planus. By courtesy of the Institute of Dermatology, London, UK.