Cronkhite-Canada syndrome
Cronkhite-Canada syndrome
Clinical features Cronkhite-Canada syndrome is a rare disorder that presents mainly in middle aged to elderly patients and is characterized by gastrointestinal polyposis, diarrhea, and malabsorption. Mortality may be high, particularly in elderly patients, due to malabsorption, malnutrition, intussusceptions, and infection. A possible association with gastrointestinal cancers, particularly gastric cancer, has been suggested.1–3 Skin changes include alopecia, nail dystrophy (in up to 98% of patients), and pigmentation, which may be diffuse or localized and macular, and predominantly involves the hands.4–7 Focal vitiligo may be seen. The nail changes consist mainly of a thin and soft triangular area in the proximal half of the nail surrounded by a thick nail plate.8 Onycholysis, onychoschizia, and onychomadesis may also be seen.8
Atrial myxomas may affect any chamber of the heart and are a very important cause of mortality, causing death in up to 25% of patients. Removal is essential to avoid death.28 Fortunately, the cutaneous markers of the disease often allow early diagnosis and treatment of the cardiac lesions.
The cutaneous myxomas are identical to sporadic superficial angiomyxomas and may present anywhere, involve the dermis and/or subcutis, have a predilection for the eyelids, external ear, and nipples, and may occur in up to 31% of patients (Fig. 20.37).29,30 They have a tendency to recur locally.6 Intraoral myxomas are exceptional.29 The lentigines affect mainly the center of the face (including the lips and conjunctiva) and occur in up to 75% or more of patients (Figs 20.38 and 20.39).31 Intraoral pigmented macules are rare (Fig. 20.40).5 Vulval lentigines are exceptional but have been documented.32 Blue nevi may occur in up to 50% of patients and are commonly seen on the trunk, face, and limbs (except for the hands and feet). They comprise ordinary blue nevi and lesions described as epithelioid blue nevi.28,33 The latter lesions are histologically identical to sporadic proliferations initially described as animal type melanoma and pigment synthesizing melanoma and more recently classified under the umbrella term pigmented epithelioid melanocytoma. These tumors are regarded as low-grade malignant with relatively frequent regional lymph node metastases but indolent clinical behavior.34 Banal nevi may also be seen.
Pathogenesis and histologic features The pathogenesis of the syndrome is unknown. Autoimmunity has been proposed as a contributing factor and some cases are associated with hypothyroidism.5,9 It has been suggested that the cutaneous signs are secondary to malabsorption, but the nail and hair changes may precede the diarrhea.4
A report of the histology from a macular area of hyperpigmentation showed increased melanin granules in keratinocytes, an increased number of melanosomes in melanocytes, and areas with an increased number of melanocytes.10
Histology of the alopecia in one case showed loss of follicular units, miniaturization of hair shafts, and deposition of glycosaminoglycans in the reticular dermis.11 A further report of two cases described diffuse anagen-telogen conversion with no inflammation or miniaturization suggesting acute telogen effluvium.12 A recent single case report suggested that the hair loss is the result of alopecia areata incognita with telogen shift and miniaturization of hair follicles.13

Fig. 20.37 Carney complex: multiple soft tumor nodules are evident on the lower trunk. By courtesy of M. Walsh, MD, Royal Victoria Hospital, Belfast, UK.

Fig. 20.38 Carney complex: numerous lentigines on the central face. By courtesy of M. Walsh, MD, Royal Victoria Hospital, Belfast, UK.
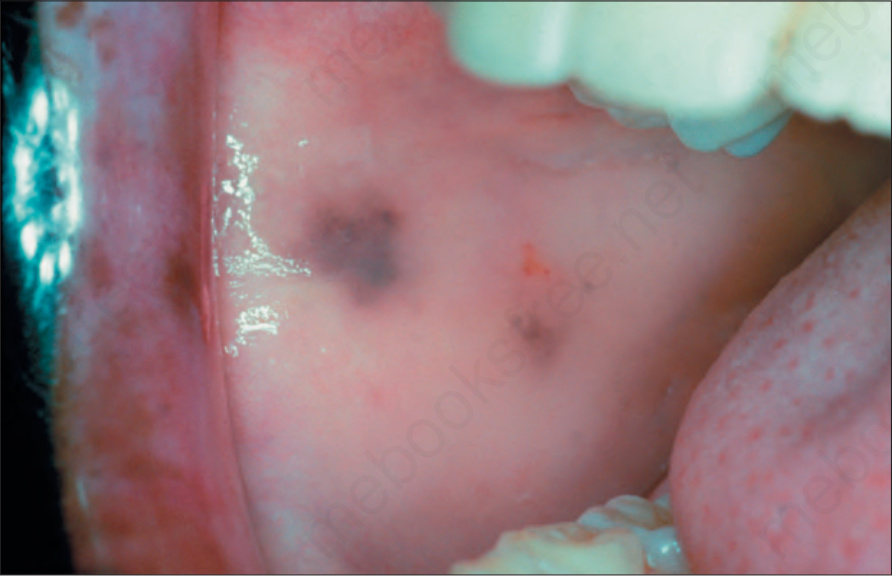
Fig. 20.40 Carney complex: pigmented macules in the oral cavity are rare. By courtesy of the Institute of Dermatology, London, UK.