Melasma
Melasma
Clinical features Melasma is a common, usually symmetric, acquired hypermelanosis characterized by irregular light- to dark-brown confluent or speckled macules with sharply demarcated margins involving sun-exposed skin; there is a marked predilection for the face (Fig. 20.23).1 A useful clinical sign not entirely specific of melasma but present within most large of lesions consists of a confetti-like macular area of regular pigmentation.2 Mild erythema is sometimes seen. Women (particularly Hispanic or Indian) are more commonly affected than men. In the latter, melasma has been reported due to estrogen therapy for prostatic cancer.3 The most common patterns are centrofacial and malar but mandibular involvement may also be seen.1,4 Presentation in other sites such as the upper limbs is uncommon and is more often described in older patients, particularly postmenopausal women on estrogen replacement therapy.5–9 It usually develops in association with oral contraceptives and pregnancy and it is triggered and worsened by sun exposure. An association has also been documented with cosmetics, phototoxic drugs, isotretinoin, anticonvulsants, and clomipramine.10 A melasma-like pigmentation has been described with imatinib.11 Exogenous ochronosis occurring in skin affected by melasma after hydroquinone use has been reported.12
of the epidermis and also melanin deposition in the superficial dermis. The type of melasma can be determined by reflectance confocal microscopy – determination of the type is important for treatment purposes. Interestingly, the elimination of melanin through the stratum corneum appears to remain the same as in normal skin.25 It is not clear whether epidermal melanocytes are increased in number, as the results of different publications are contradictory.20–26 In the dermis there is increased solar elastosis and mast cells compared to normal skin and in the papillary dermis there are often melanophages but their numbers are variable.27 Increase in the number of dermal vascular channels has also been described.28 Two very unusual cases have been reported. In one, epidermal melanocytes protruded into the dermis, and in the other, there were superficial dermal melanocytes mimicking a dermal melanocytosis.25 Prominent melanocytes protruding into the papillary dermis have been described as pendulous cells.29,30 It has been suggested that these cells are characteristic of melasma and this change may be explained by increased MMP2 expression leading to loosening of the basement membrane.30
Electron microscopy demonstrates an increase in the number of melanosomes, which are more widely dispersed in keratinocytes.21 The melanocytes show an increase in mitochondria, Golgi apparatus, rough endoplasmic reticulum, and ribosomes.
Pathogenesis and histologic features The exact pathogenesis of melasma remains unknown but there is a clear etiological link to female hormones (oral contraceptives, hormone replacement therapy, and pregnancy), UV light exposure, and family history.13,14 The hormonal relationship is further supported by the fact that men with melasma have higher circulating luteinizing hormone (LH) and low testosterone.15 Etiological mechanisms independent of sun exposure have been suggested in some studies as relevant in the pathogenesis of melasma. The latter include downregulation of the H19 gene (which encodes a 2.3-kb noncoding mRNA that plays a role in limiting body weight and cell proliferation) and reduced WIF-1 expression all resulting in stimulation of hyperpigmentation.16–18 Upregulation of PDZK1 (insulin promoter factor
- in estrogen-induced melasma has also been regarded as an important factor.19
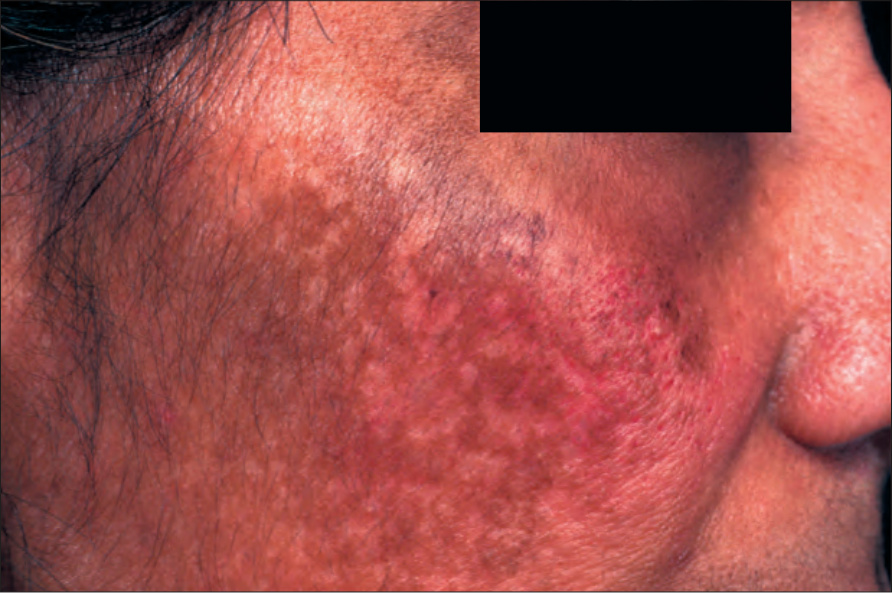
Fig. 20.23 Melasma: dark-brown macular pigmentation. By courtesy of the Institute of Dermatology, London, UK.