Progressive macular hypomelanosis
Progressive macular hypomelanosis
Clinical features Progressive macular hypomelanosis is a relatively common type of acquired patchy hypopigmentation presenting on the central trunk, mainly the back, of young adults, with predilection for females.1–4 It can affect all races, has a worldwide distribution being rare in Caucasians, and with most reported cases occurring in the Caribbean.1,5 In some Caribbean islands the disease is known as Creole dyschromia.1 The areas of hypopigmentation are well defined and vary in size but tend to be symmetrical. Over many years, lesions usually regress spontaneously.6 They are often clinically confused with pityriasis versicolor and pityriasis alba. Treatment is very difficult, but the disease is self-limiting, usually lasting no more than 3–4 years.2 A single case of a probably fortuitous association with toxic nodular goiter and another with congenital ichthyosiform erythroderma have been reported.7,8
Pathogenesis and histologic features Propionibacterium acnes may have a role in the pathogenesis of the disease.3 Follicular red fluorescence of the involved skin suggests porphyrin production by bacteria. Biopsies from involved skin have demonstrated Gram-positive bacteria in the pilosebaceous ducts with a mild perifollicular lymphocytic infiltrate. Cultures demonstrate the presence of P. acnes in lesional skin.9 However, the latter is not always present and patients with acne do not usually have progressive macular hypomelanosis. A study has demonstrated the presence of bacteria of the genus Propionibacterium but of a different as yet unidentified species than P. acnes.10 A further study, however, found an increased number of P. acnes in lesional skin by real-time polymerase chain reaction (PCR) in comparison to normal skin.11 Further reports have identified the strain P. acnes phylogenetic type III as the most commonly associated with the condition.12,13 An exceptional association with the use of antiretrovirals in HIV has been reported.14
Histology of involved skin usually shows loss of melanin in the basal cell layer of the epidermis, but the melanocytes appear normal.2,3,15
Ultrastructurally, there seems to be an increase in immature melanosomes in involved skin compared to normal skin.4 There is a switch from stage IV (negroid) melanosomes to small type I–III aggregated melanosomes (caucasoid).2

Fig. 20.20 Hypomelanosis of Ito: whorled hypopigmentation on trunk and limbs. By courtesy of the Institute of Dermatology, London, UK.
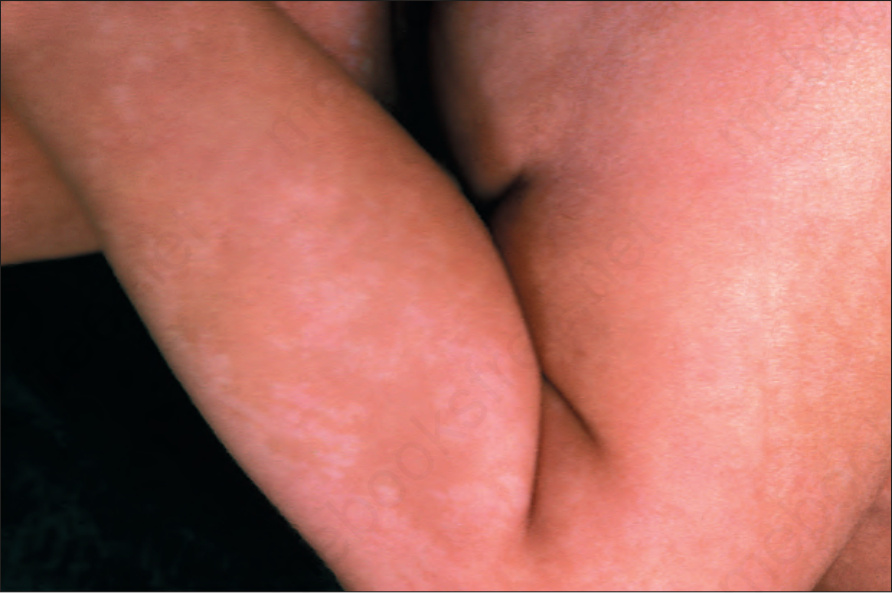
Fig. 20.21 Hypomelanosis of Ito: detail of whorled hypopigmentation in a limb. By courtesy of the Institute of Dermatology, London, UK.