Vitiligo
Vitiligo
Clinical features Vitiligo is a common acquired disease of unknown etiology characterized by loss of melanocytes resulting in macular areas of leukoderma that progressively enlarge and often become confluent.1–4 The incidence has been calculated as between 1% and 2% of the population.5,6 It affects all races but appears to be more common in people with dark skin. However, the latter may represent an overestimate, as the disease tends to be more noticeable in patients with darker skin. The sex incidence is equal, with a peak incidence between the ages of 10 and 30 years (up to 50% of cases). The disease is also seen in the very young and the elderly.7–10 In children, the mean age of onset is 6 years and there appears to be a slight predilection for females.9 Between 25% and 40% of patients have a positive family history of the disease; inheritance is non-mendelian, multifactorial, and polygenic.6,11,12 In patients with a positive family history the disease usually appears earlier in life.6 The frequency of the disease in siblings of affected patients is about 18 times that encountered in the general population.6 Vitiligo affects monozygotic twins concordantly in about 23% of cases.6
suggestive of mosaicism and presentation is in the first decades of life, with predilection for the face, early leukotrichia, and rapid progression followed by stabilization.16 Generalized disease may be associated with segmental involvement in what is referred to as mixed pattern vitiligo and the latter is more commonly associated with halo nevi and leukotrichia.19,20 Focal vitiligo is defined as a nonsegmental isolated lesion usually several centimeters in diameter.16–18 Mucosal vitiligo is restricted to oral mucosa and genitals. In vitiligo, the skin over bony prominences is commonly affected, suggesting that repeated trauma may play a role. Involvement of flexural areas, genitalia, and the skin around the eyes and mouth is also frequently seen (Fig. 20.3). Premature graying of the hair is a common event and occurs even in children. Affected areas are prone to sunburn and the Koebner phenomenon may be seen (Fig. 20.4). Early lesions can have an erythematous ‘inflammatory’ border and in a minority of cases focal peripheral hyperpigmentation is a feature. Some patients describe mild pruritus in the early stages of the disease. The hairs within affected areas tend to remain pigmented but may lose the pigment in late stages (Fig. 20.5). A tanned zone between pigmented and completely nonpigmented skin is detected in some patients with darker skin. Known as trichrome vitiligo,21,22 it tends to indicate the presence of active disease.21 Activity is also indicated by inflammatory and confetti-like lesions. An unusual variant of inflammatory, figurate papulosquamous vitiligo has been documented.23 Vitiligo can also develop in individuals exposed to phenolic compounds, particularly in cleaning solutions.24 Patients may develop halo nevi (see Fig. 20.4) or vitiligo may develop after the development of halo nevi.25,26 Generalized complete depigmentation is exceptional. Spontaneous repigmentation may be seen but it is patchy and tends to concentrate in perifollicular skin (Fig. 20.6). A case of repigmentation of
The progression of vitiligo is slow and it is common for lesions to start on sun-exposed skin and usually with a symmetrical distribution (Figs 20.1 and 20.2).13,14 Stress has been suggested as a precipitating event in vitiligo in a number of patients.15 In a minority of cases involvement is unilateral. Segmental vitiligo refers to a variant of the disease presenting with linear or block-like distribution and erroneously described in the past as dermatomal.16–18 The distribution of lesions in this type of vitiligo is more
991 Vitiligo
vitiligo after a beetle dermatitis has been documented.27 Patients with the disease occasionally have uveitis, and an association with deafness has also been reported.28,29
Some patients with vitiligo develop actinic keratoses and squamous cell carcinomas on sun-exposed areas affected by the disease.30,31 This occurrence is, however, not as high as might be expected and may be due to
inadequate sun protection. Patients treated with psoralen plus ultraviolet light of A [long] wavelength (PUVA) may be more prone to develop skin cancer in the involved skin.32
Polymorphic light eruption lesions limited to areas of skin involved by vitiligo has been described.33 Allergic contact dermatitis may exceptionally present as vitiligo.34
Vitiligo can be associated with numerous diseases, particularly (but not exclusively) those with a clear or suspected autoimmune basis. Autoimmune diseases may be seen in up to a third of patients with vitiligo. Patients with generalized vitiligo are more likely to have autoimmune disease. The latter associations include thyroid disease (hypo- and hyperthyroidism and Hashimoto disease), diabetes mellitus, Addison disease, and (much less commonly) alopecia areata, acanthosis nigricans, dermatitis
992 Disorders of pigmentation
in a patient of North European extraction.66 Vitiligo may rarely occur at the site of radiotherapy.67,68 A single case of Baboon syndrome (systemic contact dermatitis as a result of inhalation of mercury vapor) with segmental vitiligo has been reported.69 Patients with melanoma rarely develop areas of leukoderma, not only around the tumor but also away from it and in association with metastasis.70–74 Poliosis may also occur. Of note, it has been suggested that the prognosis is better in patients with leukoderma and melanoma.72 It is controversial whether the depigmentation seen in patients with melanoma represents vitiligo.71
Rarely, a number of drugs have been associated with vitiligo. These include chloroquine, ganciclovir, interferon-alpha (IFN-α), tolcapone, levodopa, PUVA, and imiquimod.72–83 Vitiligo has also occurred following narrow-band TL-01 phototherapy for psoriasis, at a site of allergic contact dermatitis to nickel, and after intense pulsed light treatment.84–86 The disease has also been induced by a lymphocyte infusion in a patient with relapsed leukemia and there is a report of an exceptional case of transfer of vitiligo after allogeneic bone marrow transplantation.87,88
Pathogenesis The pathogenesis of vitiligo remains obscure and there are a number of theories as to why the epidermal melanocytes are destroyed. It is likely that the disease is multifactorial, has an autoimmune basis, and in a number of cases, involves a genetic predisposition. Environmental factors may also be associated with the causation of the disease. Several of the mechanisms proposed are probably involved simultaneously.89,90 They are likely to be interrelated and often, genetic predisposition plays a role. The inheritance is polygenic. Around 50 gene loci have been identified in association with vitiligo risk in genome-wide association and genetic linkage studies. The genes are associated with innate immunity or adaptive immunity, or are only related to melanocytes.17,91,92
herpetiformis, pernicious anemia, spondyloarthritis, and pemphigus vulgaris (Fig. 20.7).35–45 The most frequent associations are with thyroid autoimmune disease, autoimmune gastritis, and alopecia areata.46 Patients with Grave disease or Hashimoto thyroiditis have a risk of more than 10-fold of developing vitiligo.47 Other reported associations of vitiligo include sarcoidosis, Crohn disease, morphea, lichen sclerosus, actinic granuloma, chronic mucocutaneous candidiasis, 20-nail dystrophy, chronic actinic dermatitis, psoriasis, lepromatous leprosy, AIDS, MELAS (mitochondrial encephalomyopathy, lactic acidosis and stroke-like episodes syndrome), frontoethmoidal meningoencephalocele, dysgammaglobulinemia, phakomatosis pigmentovascularis type IIa, and idiopathic CD4+ T-cell lymphocytopenia.43,48–64 Unilateral involvement in association with trigeminal autonomic cephalalgia has also been described.65 The vitiligo-spasticity syndrome seems to be a distinctive syndrome, mainly described in Arab patients but also documented
The autoimmune hypothesis is based on the observation that patients with vitiligo have an associated autoimmune disease in 15% to 30% of cases.15,35 Affected patients are also frequently found to have autoantibodies to gastric parietal, thyroid, and adrenal cells.93 Antibodies to normal melanocytes have been reported in patients with vitiligo.94–96 The level of these antibodies in the serum appears to correlate with disease activity.95,97 Important links have been shown between generalized vitiligo and single-nucleotide polymorphisms at several loci associated with autoimmune diseases.97 Interestingly, one of these associations is with a locus containing TYR, which encodes tyrosinase. A mutually exclusive relationship between the tendency to develop vitiligo and susceptibility to melanoma has been suggested.98 Both antibody-dependent, cell-mediated cytotoxicity and direct destruction of melanocytes by antibodies have been proposed as mechanisms.95,99 Although it was initially suggested that the antibodies
993 Vogt-Koyanagi-Harada disease
in the serum of patients are directed against tyrosinase, this view has been challenged.100–103 The activation of natural killer (NK) cells by antibodies does not seem to play an important role in some studies.104,105
An important theory in the pathogenesis of vitiligo is referred to as the self-destruction theory.106 This proposes that melanocytes are destroyed not only by toxic melanin precursors, such as free radicals, but also by melanin itself in predisposed individuals.107 It is not clear, however, why these toxic melanin precursors and melanin affect the melanocytes in some individuals and not in others, but it may be that the mechanism for their disposal is faulty in patients who develop vitiligo. Experimental evidence is based on the fact that a number of chemicals, including phenols like monobenzyl ether of hydroquinone, induce pigmentary changes indistinguishable from vitiligo.108 It has also been demonstrated that death of melanocytes in vitiligo results from increased sensitivity to oxidative stress.109 The group of enzymes known as glutathione transferases is involved in protecting cells against toxic chemicals. Interestingly, it has been shown in a Chinese population that patients with GSTT1 and GSTM1-null genotypes have increased risk of developing vitiligo as compared to those that exhibit GSTP1 polymorphisms.110 It has been proposed that an alteration in the membrane lipids of vitiligo cells after stress leads to mitochondrial damage and production of reactive oxygen species.111 Thioredoxin domain containing 5 (TXNDC5) polymorphisms has been associated with the development of nonsegmental vitiligo in Korean patients.112 TXNDC5 is a member of the thioredoxin family and its function resides in protein folding and chaperone activity against endoplasmic reticulum stress induced by oxidative stress. It is likely that affected cells activate inflammatory signals leading to the triggering of innate immunity by dendritic cells and NK cells, the former of which present melanocytic antigens to T cells. Melanocyte-specific CD8-positive T cells play a very active role in the destruction of melanocytes.17,113,114 IFN-gamma seems to play a crucial role in the recruitment of CD8-positive T cells through the induction of CXCL10 and its receptor CXCR3.115–117
skin was found in one study.122 Other reported changes include increased numbers of Langerhans cells, epidermal vacuolization, and thickening of the basal membrane.123 The loss of pigment and melanocytes in the epidermis is highlighted by a Masson-Fontana stain and by immunohistochemistry (Fig. 20.9). To avoid confusion with Langerhans cells (which are also S-100+) other melanocyte markers such as Melan-A and particularly microphthalmia transcription factor 1 (MITF1) or SOX10 (both expressed in the nuclei of melanocytes) may be used. Although both CD4- and CD8-positive cells are found within the infiltrate in active lesions, CD8-positive cells seem to predominate, appear to be associated with the damage at the dermal– epidermal junction, and are associated with the severity of the disease.124,125 This has been shown both in generalized and segmental vitiligo.
Differential diagnosis Distinction from guttate hypomelanosis is based on clinical presentation and on the complete absence of melanocytes in vitiligo, and the persistence of at least some melanocytes in the former. Distinction from postinflammatory hypopigmentation is based on the preservation of melanocytes with only loss of pigment in the latter. In the inflammatory stages of vitiligo, changes may mimic cutaneous T-cell lymphoma and distinction can be very difficult without close clinicopathological correlation.

Fig. 20.1 Vitiligo: symmetrical involvement of the upper limbs. By courtesy of the Institute of Dermatology, London, UK.

Fig. 20.2 Vitiligo: symmetrical involvement of the body. Note patchy repigmentation secondary to PUVA treatment. By courtesy of the Institute of Dermatology, London, UK.

Fig. 20.3 Vitiligo: genital involvement is often seen in vitiligo. By courtesy of the Institute of Dermatology, London, UK.

Fig. 20.4 Vitiligo: area of hypopigmentation due to the Koebner phenomenon and the presence of a halo nevus. These are frequent findings in vitiligo. By courtesy of the Institute of Dermatology, London, UK.
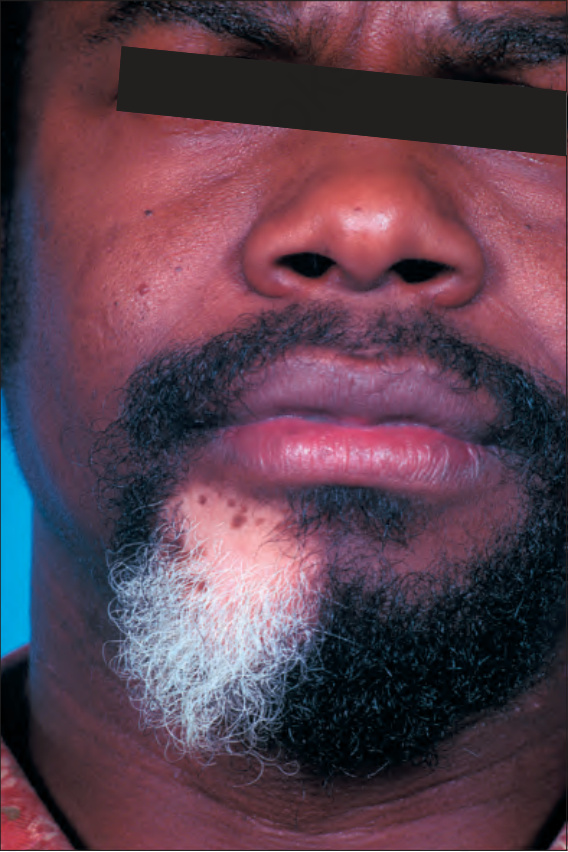
Fig. 20.5 Vitiligo: development of gray hair in a longstanding patch of vitiligo. By courtesy of the Institute of Dermatology, London, UK.
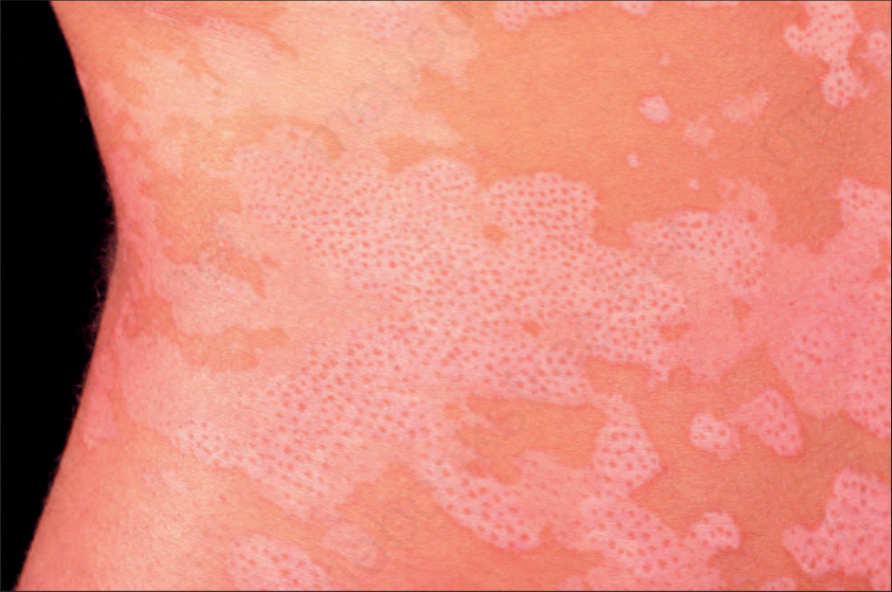
Fig. 20.6 Vitiligo: repigmentation in vitiligo frequently has a perifollicular distribution. By courtesy of the Institute of Dermatology, London, UK.

Fig. 20.7 Vitiligo: coexistence of vitiligo and alopecia areata. By courtesy of the Institute of Dermatology, London, UK.
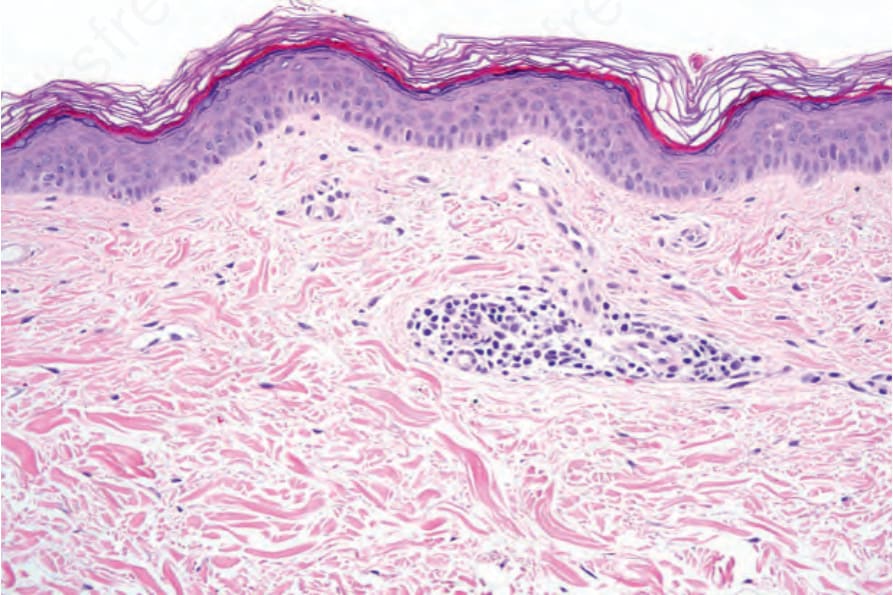
Fig. 20.8 Vitiligo: skin biopsy from lesional skin stained with hematoxylin and eosin. There is complete absence of melanocytes and melanin pigment. There is a light perivascular chronic inflammatory cell infiltrate.
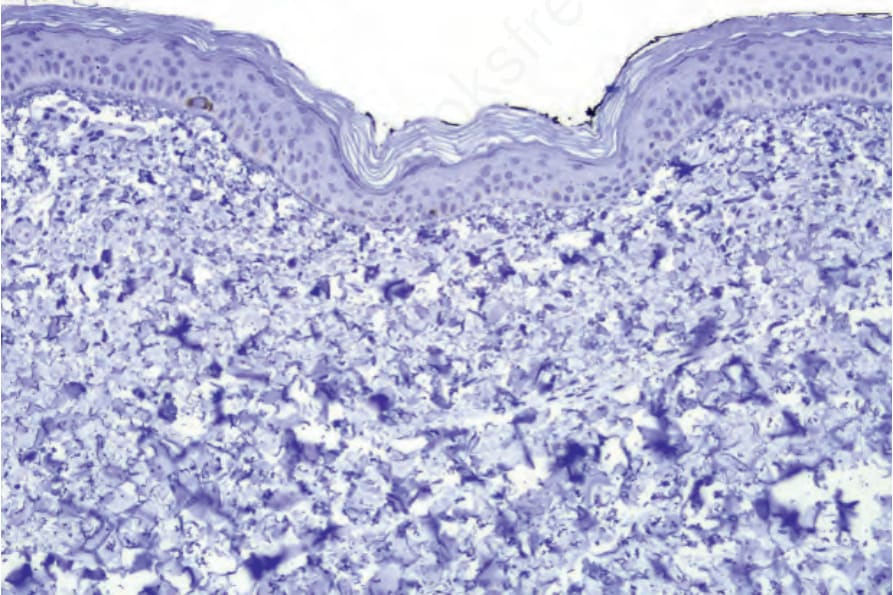
Fig. 20.9 Vitiligo: skin biopsy from lesional skin stained with S-100 protein. A single residual positive cell is present.