Bacterial infections
Bacterial infections
Individuals with HIV have high a higher rate of skin and soft tissues infections (SSTIs).1 Group A streptococci and S. aureus may be causative organisms in cellulitis, impetigo, necrotizing folliculitis, furunculosis, pyoderma, and erysipelas. S. aureus is the most common bacterial pathogen in patients with HIV. It may present as botryomycosis.2 Bacterial folliculitis can also be a feature of HIV infection. It presents as an acneiform eruption affecting the face, back, chest, and buttocks or else as a relapsing condition in the axillae.3 Histologically, bacterial folliculitis is characterized
987.e1 Cutaneous infections
A
B
988 Human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS)-associated cutaneous diseases
by a purulent exudate within the follicular epithelium accompanied by a surrounding lymphohistiocytic infiltrate.3 Plasma cells and eosinophils may also be evident.
The incidence of community-associated methicillin-resistant Staphylococcus aureus (MRSA) is increased in individuals with HIV infection and is a risk factor for recurrent SSTIs.4 S. aureus strains in HIV infected individuals often carry the Panton-Valentine leukocidin, which is associated with severe necrotizing infections.5,6
Bacillary angiomatosis is a vasoproliferative lesion induced by infection with either Bartonella henselae or B. quintana.7 Patients with CD4 lymphocyte counts of less than 100 cells/mm3 are at risk.8
Dermatophyte infections (e.g., tinea pedis, tinea cruris, and tinea capitis) and onychomycosis often become very severe and extensive. Disseminated mycoses caused by Cryptococcus neoformans, Histoplasma capsulatum, Coccidioides species, and Talaromyces (Penicillium) marneffei and pneumonia due to Pneumocystis jirovecii are indicator conditions of advanced HIV disease.2 Other fungi causing systemic or cutaneous infection in association with HIV include Paracoccidioides brasiliensis, Aspergillus species, and Mucor species Sporothrix schenckii.3,4
An interesting and unusual observation has been the identification of P. jirovecii in middle ear infections presenting as polyps within the external auditory meatus in a patient who subsequently developed pulmonary involvement.5 Histologically, these lesions showed features similar to those seen in pulmonary lesions.
HIV-infected individuals with Mycobacterium tuberculosis infections may have varied features on histology from noncaseating granulomata to caseating granulomata to an absence of granulomata.9 In infection with the nontuberculous mycobacteria Mycobacterium avium complex (MAC), the features may be granulomatous, but more commonly consist of a nongranulomatous infiltrate of neutrophils, numerous foamy macrophages, lymphocytes, plasma cells, and eosinophils (Figs 19.33–19.37).9 Skin lesions due to MAC are rare and usually represent disseminated disease.9 Mycobacterium kansasii infection may result in a spindle cell ‘proliferative’ lesion reminiscent of the histoid variant of lepromatous leprosy.10 The presence of more typical foamy macrophages is a useful diagnostic discriminant.
Syphilis is associated with increased acquisition of HIV. Data from the CDC in 2014 showed that approximately 40% of individuals diagnosed with syphilis were HIV infected.11 False-negative RPR/VDRL tests due to the prozone phenomenon and delayed seroreactivity may be more common in HIV-infected individuals.12
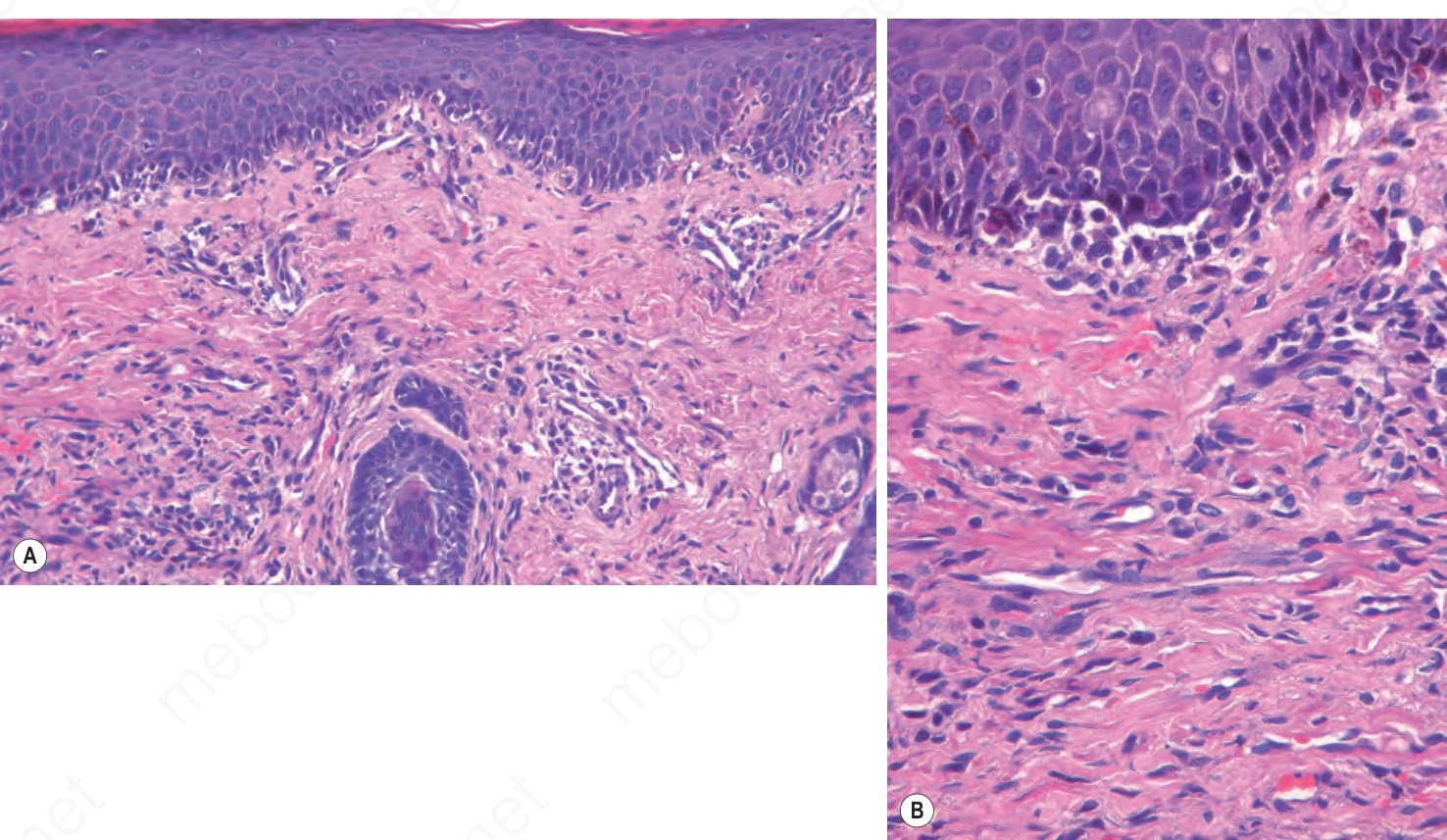
Fig. 19.32 AIDS interface dermatitis: (A) this field shows the features of patch-stage Kaposi sarcoma with overlying interface change; (B) high-power view.
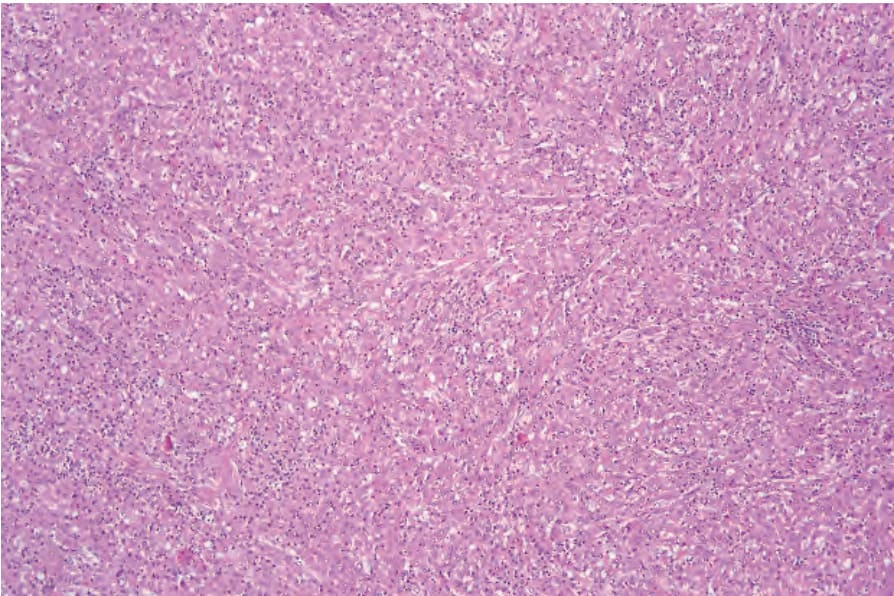
Fig. 19.33 HIV-associated Mycobacterium avium intracellulare infection: within the dermis is a diffuse macrophage infiltrate.