Xerosis
Xerosis
Clinical features Xerosis is common in HIV infection, occurring at any time throughout disease progression but significantly associated with lower CD4 counts and the ART drug indinavir.1,2 Xerosis is often pruritic but less so than other HIV associated dermatoses.3 Xerotic dermatitis was reported by 42.1% of men and 51.5% of women infected with HIV in the FRAM study.2 It is characterized by diffuse dryness of the skin with hyperpigmented scales and
980 Human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS)-associated cutaneous diseases
focal crusting (Fig. 19.13).1,4 It is often prominent on the extremities and is worse in the winter months. Affected skin may fissure, leading to eczema craquelé and secondary infection in some patients. Occasionally, discrete thickened patches occur.1
Pathogenesis and histopathology The pathogenesis of xerosis, although obscure, may be related to a range of factors, including cutaneous microcirculation and nutritional alterations, altered sweat or sebaceous gland activity, alterations in the composition of sweat, and changes in the cutaneous mast cell population. Decreased calcitonin gene-related peptide and substance P levels have been documented in HIV-associated xerosis.5 Epidermal lipid content has been shown to be reduced in individuals with HIV.6 These factors may result in decreased epidermal integrity, with a resultant reduction in the effectiveness of the epidermal barrier.5
Skin biopsies often demonstrate minimal superficial epidermal hyperkeratosis with parakeratosis, mild acanthosis, and focal spongiosis in the absence of microvesiculation (Fig. 19.14). The dermis demonstrates a minimal perivascular lymphocytic infiltrate. An inconsistent finding is the presence of
early alterations of acquired ichthyosis, characterized by dense orthokeratosis with a diminished granular cell layer and minimal inflammation. Other pruritic scaling dermatoses, such as scabies, dermatophytosis, and the ‘flaky skin’ appearance of kwashiorkor, are clinicopathological mimickers, as all of these conditions may occur in individuals with advanced HIV infection.1
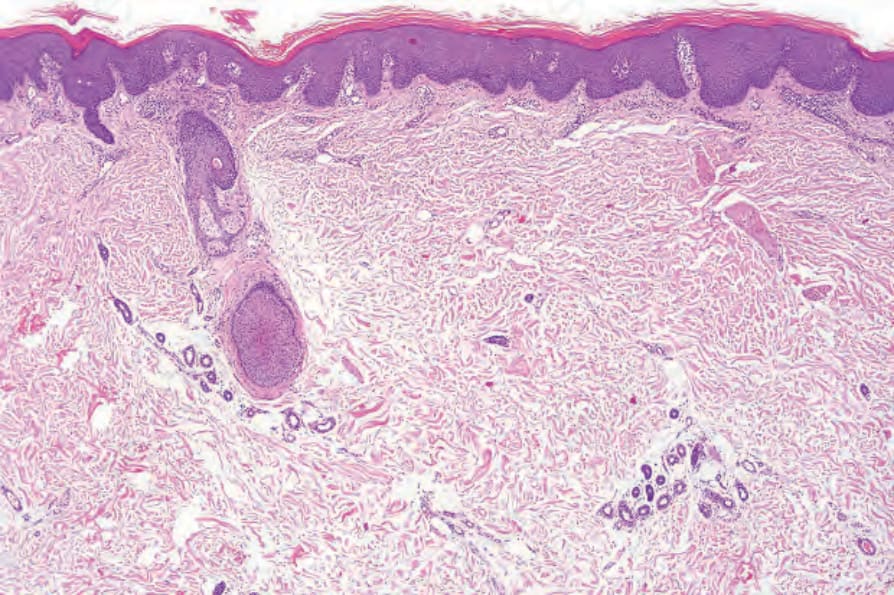
Fig. 19.11 HIV-associated pityriasis rubra pilaris: low-power view showing a thickened stratum corneum and psoriasiform hyperplasia.
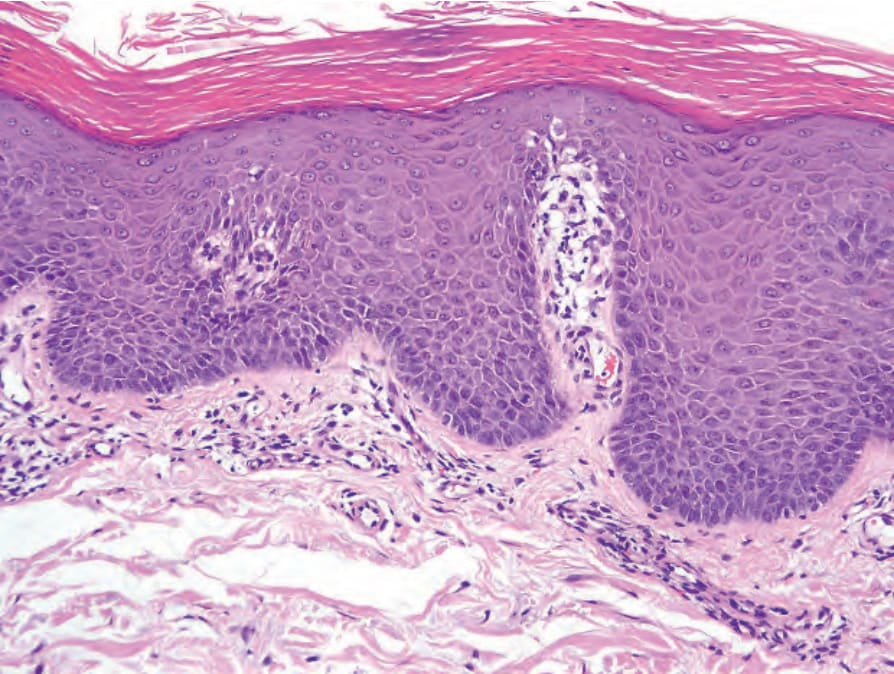
Fig. 19.12 HIV-associated pityriasis rubra pilaris: there is alternating orthohyperkeratosis and parakeratosis.

Fig. 19.13 HIV-associated xerosis: marked scaling has resulted in an eczema craquelé-like appearance. Dry skin is a common complaint in patients with HIV infection. By courtesy of C. Furlonge, MD, Port of Spain, Trinidad.
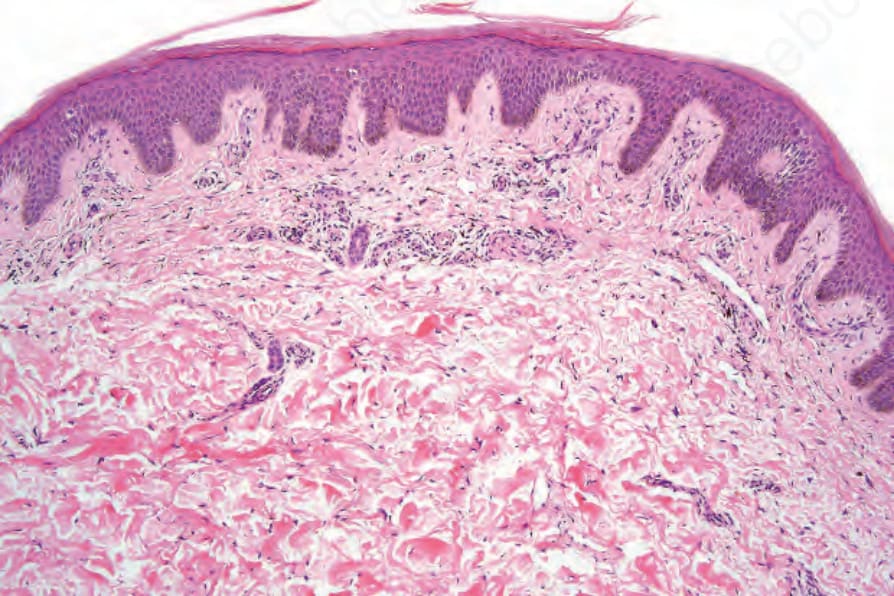
Fig. 19.14 HIV-associated xerosis: there is hyperorthokeratosis and parakeratosis associated with psoriasiform hyperplasia. There is only minimal spongiosis on the right side of the figure.