Rhinosporidiosis
Rhinosporidiosis
Clinical features Rhinosporidiosis is an uncommon and somewhat enigmatic disease caused by Rhinosporidium seeberi, an organism that until relatively recently was considered to be a fungus, based on its morphological and staining characteristics.1,2 Molecular biological analysis, however, has since revealed that the causative agent is a novel aquatic protistan Ichthyosporean microbe and member of a new clade termed the Mesomycetozoea.3–5 This new class is located at the animal-fungal boundary, and its members include ten other parasitic and saprobic microbes.3,4,6 The etiological agent was briefly renamed Microcystis aeruginosa in 2001 after it was cultured for the first
time.2,7–11 Infection results in polypoid lesions containing characteristic cyst-like sporangia.7
Rhinosporidiosis is found in India and Sri Lanka as a waterborne infection affecting mainly the nasopharynx, and as a dustborne infection affecting equally conjunctiva and nasopharynx in the dry southern states of the United States. Sporadic cases have been reported worldwide.1 Multiple host-specific strains may exist.6 The infection affects men much more commonly than women and presents as hyperplastic polypoid mucosal lesions.12 Lesions in the nose resemble ‘allergic’ nasal polyps. The same polypoid presentation is seen in the lesions of the conjunctiva. In one recent series of ocular rhinosporidiosis reported from India, more than half of those afflicted were children aged less than 10 years.13 The infection occasionally involves the larynx, trachea, and the mucosae of the rectum, urethra, and
genitalia, where it resembles condylomata.1,14–17 Other rarely reported sites include the vagina, the pinna and the lacrimal sac.18–20
Exceptionally rarely, disseminated variants have been recorded.12,21–30 Disseminated disease manifests with widespread cutaneous or subcutaneous nodules, plaques, soft tissue masses, or even osteolytic bone lesions.21–25,28,30,31 Rarely, cutaneous lesions in disseminated disease may be associated with a verruciform appearance or an overlying cutaneous horn.30,32 Pulmonary involvement and involvement of the nail apparatus have also been reported.33,34 Primary cutaneous lesions are rare and are described as papules which become verrucous and granulomatous.7,35 Giant cutaneous or subcutaneous lesions mimicking soft tissue tumors have also been described.36–40
965 Rhinosporidiosis
Pathogenesis and histologic features The precise mechanism of infection is unknown. It has been proposed that the organism is present in soil, dust, and water and that involvement of the nose and conjunctiva follows rubbing with contaminated fingers.1 Cutaneous involvement occurs by contiguous extension from a mucosal infection, autoinoculation, and rarely through hematogenous dissemination.22,41,42 The presence of significant antirhinosporidial antibody titers does not appear to confer a protective effect.43 It has been shown that synchronous nuclear divisions take place in the juvenile and early intermediary sporangia of R. seeberi, without cytokinesis; this results in the formation of thousands of nuclei. Cytokinesis, however, occurs as a one-time event in the latest stages of intermediate sporangia, immediately prior to the development of mature sporangia.5
In tissue, the causative agent is characterized by thick-walled (birefringent) endospore-filled sporangia.1 These are seen in the stroma of the polyps as cysts, 10–200 µm in diameter (Figs 18.378 and 18.379). The cysts have a thick wall, which remains in a collapsed form after the endospores have been released. Endospores are seen initially at the periphery of the sporangium, but they gradually fill the cyst-like center before rupture occurs. The spores are 7–8 µm in diameter and contain 8–10 eosinophilic globular bodies (Fig. 18.380). They mature to form small trophic cysts (Fig. 18.381). The lesions are easily identified on H&E-stained sections and can also be demonstrated by PAS and methenamine silver stains.12 Watery substances stimulate mature sporangia to undergo rupture, with subsequent discharge of the endospores. This affinity for wet environments may also explain why infections tend to involve the mucous membranes of human hosts.1
The cysts are associated with a stromal mixed neutrophil, histiocyte, plasma cell, and lymphocyte infiltrate. The overlying epidermis in skin lesions may show pseudoepitheliomatous hyperplasia, hyperkeratosis, and papillomatosis.1 Foreign body giant cells may be abundant. These may sometimes assume gigantic proportions, with engulfed sporangia.37
966 Infectious diseases of the skin
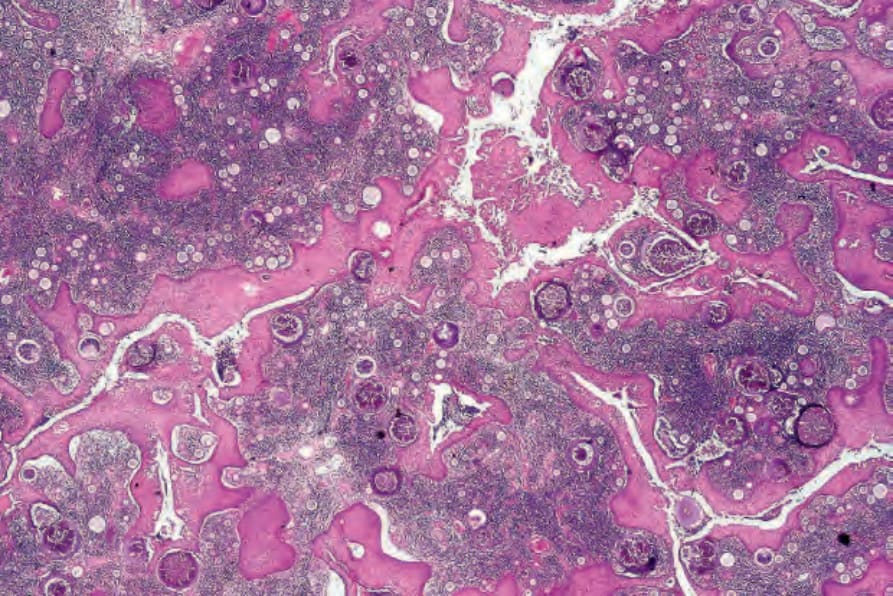
Fig. 18.378 Rhinosporidiosis: this is part of a polypoid nasal lesion. Multiple sporangia containing conspicuous spores are present.
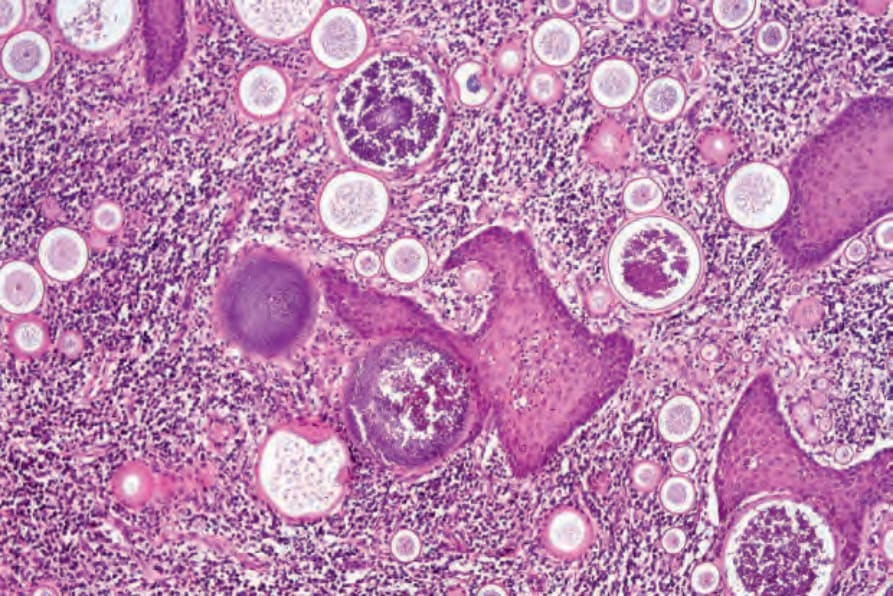
Fig. 18.379 Rhinosporidiosis: maturation of the spores is from the periphery to the center of the cyst; note the thick hyaline eosinophilic wall.
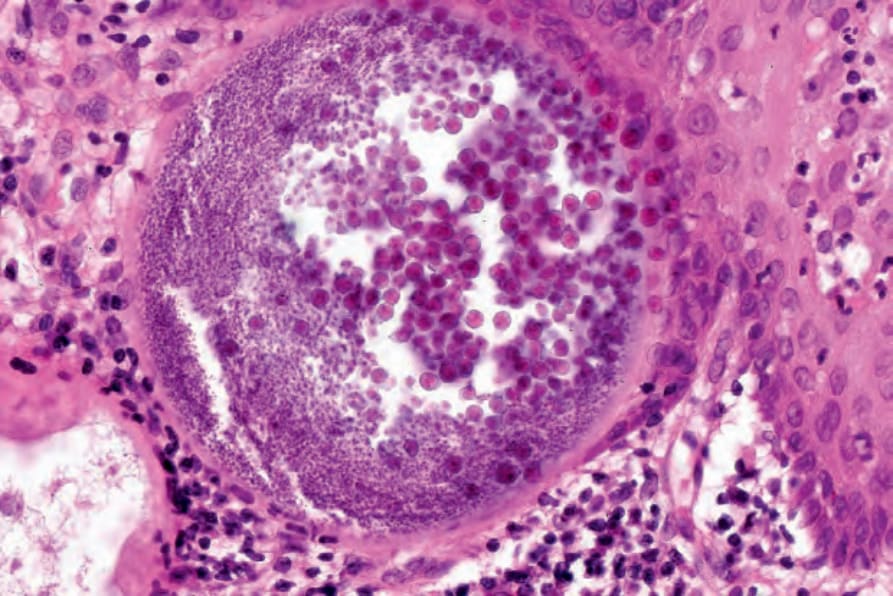
Fig. 18.380 Rhinosporidiosis: high-power field showing the internal structure of the spore.
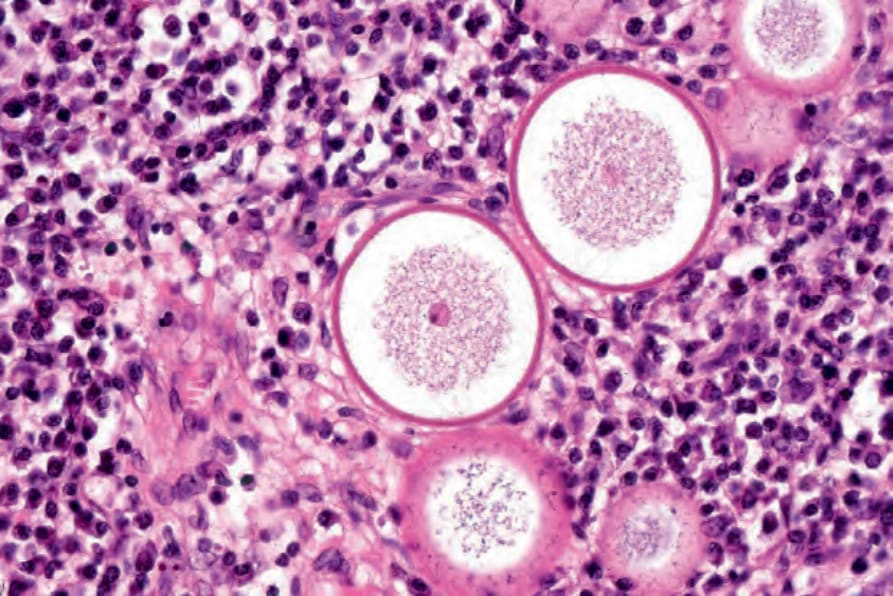
Fig. 18.381 Rhinosporidiosis: individual spores mature to form small trophic cysts.