Pneumocystosis
Pneumocystosis
Clinical features Pneumocystosis is an infection caused by the fungus P. jiroveci (formerly P.carinii), which for decades was considered to be a protozoal organism.1–3 Although pulmonary disease is well described in immunocompromised individuals, especially those with HIV/AIDS, skin involvement is distinctly uncommon.4–10 Almost all examples of cutaneous pneumocystosis have been associated with HIV/AIDS, where the condition may serve as a sentinel of underlying HIV/AIDS infection.4–13 Skin infection is often not accompanied by pulmonary pneumocystosis.5,7,10,12,14 The presence of persistent cough, fever, and an abnormal chest radiograph, however, infers concomitant lung infection.5
A
Cutaneous P. jiroveci infection manifests with one or multiple polypoid masses in the external auditory canal in a vast majority of cases. Otorrhea is a frequent symptom.4,8–11,14 Potential complications include perforation of the tympanic membrane, destruction of the mastoid bone, cranial nerve involvement, and rarely, extension of the disease to involve the middle cranial fossa.8,9 On occasion, however, non-otic skin lesions may occur, manifesting as a non-specific rash, cutaneous nodules, umbilicated MC-like translucent papules, one or more macules, brownish facial papules and plaques, or lesions resembling Kaposi sarcoma.5–7,15 Potential sites of involvement include glabrous skin and the axilla.5,7 Primary infection of the conjunctiva of the upper eyelid has also been reported.16
Histologic features In most otic examples, there is a proliferation of granulation tissue accompanied by a mixed inflammatory cell infiltrate and a distinctive foamy exudate that is not too dissimilar to that encountered in cases of pulmonary pneumocystosis (Fig. 18.377).10,16 This exudate is easily overlooked and a high index of suspicion should thus be maintained. The exudate may exhibit a propensity to be concentrated around vessels, and in some cases there is a surrounding granulomatous reaction with multinucleated giant cells.10 Fibrin deposition is observed within and around blood vessels. Sections stained with the Gomori methenamine silver method will usually highlight the characteristic cup-shaped yeasts amid the frothy exudate.10,16 Indirect immunofluorescence or electron microscopy may also be employed to confirm the diagnosis.13,16 The organism is notoriously difficult to culture.
B
There have been isolated reports of dual infection with other organisms, including botryomycosis due to concomitant Staphylococcus aureus infection, and skin lesions harboring both Pneumocystis organisms and Cryptococcus neoformans.12,13, A unique case of the latter showed both organisms within the cytoplasm of foamy histiocytes, and a resultant picture closely mimicking a xanthoma.15
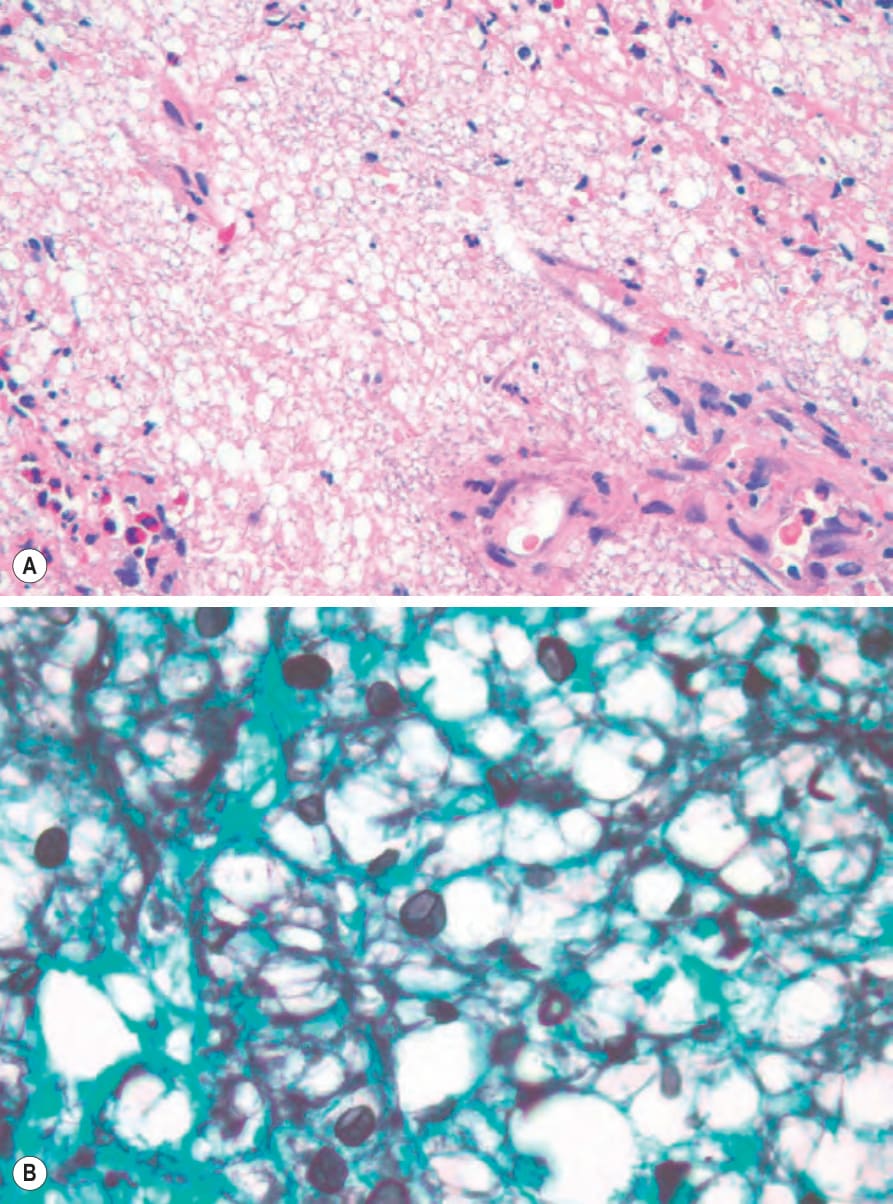
Fig. 18.377 Pneumocystis infection: (A) within the dermis is a diffuse ‘bubbly’ infiltrate; (B) the methenamine silver stain shows the typical morphology. By courtesy of T. Madliwa, MD, Lancet Laboratories, Johannesburg, South Africa.