Lobomycosis
Lobomycosis
Clinical features Lobomycosis is a very rare infective dermatosis caused by the fungus Lacazia loboi (formerly Paracoccidioides loboi or Loboa loboi).1–5 The disease was first described by Jorge Lobos in Recife, Brazil, in 1931.5,6 Although culture is exceedingly difficult, the organism has been successfully inoculated into mice, rats, and armadillos.7 It is generally confined to tropical forest areas of Central and South America, especially the Amazon basin.2,3,6,8–10 The first case of lobomycosis in the United States was reported in 2000 and additional rare cases have been recorded in North America since then.11,12 Rare infections have also been described in African patients. Although the natural habitat of the fungus remained an enigma for many years, soil and vegetation are now believed to be the main habitat.13 Infections in dolphins were later reported, suggesting the possibility of a waterborne mechanism of spread, and implied zoonotic transmission.13–15 Furthermore, affected dolphins have been found to have impaired adaptive immunity.16 More recent epidemiological evidence, however, suggests that direct or indirect transmission of the fungus from dolphins to humans is an exceedingly rare event.15
inoculation of the skin, and present characteristically after many years. They occur on exposed skin, often on the face and earlobes, but the arms, chest, back, legs, buttocks, or lumbosacral region may also be affected (Figs 18.373 and 18.374). Lesions are associated with keloid-like scarring, hence the diseases previous designation ‘keloidal blastomycosis’.1,3,8,11,17,18 There are usually papular, nodular, and verrucous components; some of the nodules may become large and confluent, and ulceration sometimes occurs. Drainage lymph nodes are affected.18–20 Although the lesions are usually painless, pruritus, hypoesthesia, burning, or anesthesia can occur.18 There is no tendency to heal and the infection is resistant to medical therapy, leaving surgical excision as the sole effective treatment. Disseminated cutaneous lesions may occur, sometimes following local relapse.21–23 Squamous carcinoma is an occasional long-term complication.9,24
The disease is seen in whites, blacks, and native South American Indians, and particularly affects males.2,3,7 Lesions due to this fungus are mainly confined to the skin, but contiguous subcutaneous involvement may occur.10 They are extremely insidious in development, following presumed traumatic
Histologic features The fungus presents in the tissues as characteristic bulbous chains of yeast-like cells, 6–12 µm (generally 9–10 µm) in diameter, with thick (double) walls and interconnecting tubular structures which later disappear.10,14,18 Budding forms are occasionally present.18
Cutaneous involvement by L. loboi provokes a distinctive reaction. The infection is centered on the dermis, which becomes infiltrated by fungus-containing foamy histiocytes and giant cells, with the latter predominating centrally (Figs 18.375 and 18.376). Few other inflammatory cells are evident and fibroblasts appear later within the surrounding keloid. Suppurative inflammation and necrosis are absent. The fungi are unstained and seen
963 Lobomycosis
A
B
964 Infectious diseases of the skin
easily with H&E staining, but PAS and methenamine silver stains enhance their recognition. The overlying epidermis is generally attenuated, although vegetating lesions are associated with hyperplasia and hyperkeratosis. Transepidermal elimination of the organisms may occur.18 In heavily infected lesions, skin appendages and nerves can be destroyed, and therefore the condition can clinically mimic leprosy. Interestingly, there have been isolated reports of co-infection with leprosy and lobomycosis.25 Recent studies have highlighted the role of regulatory T-cells in the host immune response in lobomycotic skin lesions.26,27
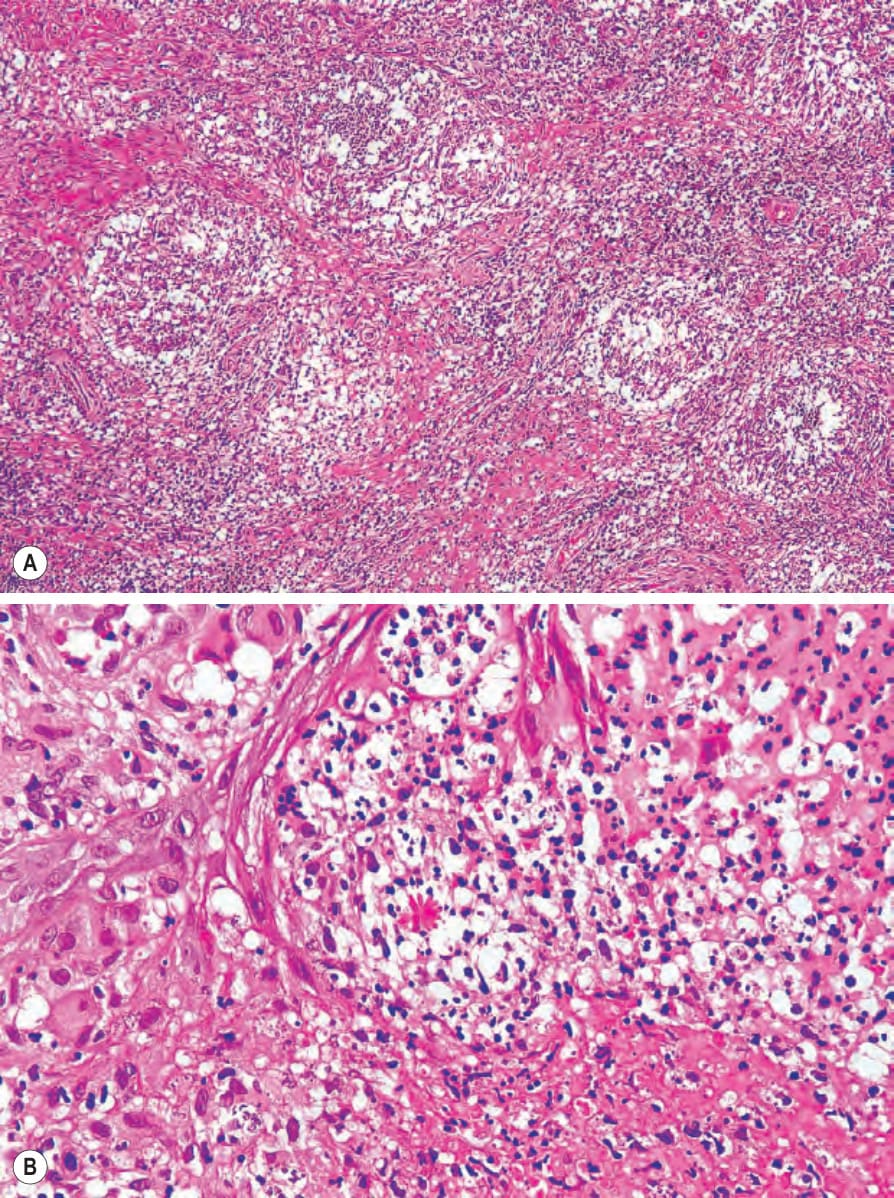
Fig. 18.372 (A, B) Sporotrichosis: multiple dermal abscesses are typically present in this condition.

Fig. 18.373 Lobomycosis: the ear is a commonly affected site. By courtesy of S.A. Pecher, MD, Centro Manaus, Amazonas, Brazil.

Fig. 18.374 Lobomycosis: note the gross keloidal scarring with considerable disfigurement. By courtesy of S.A. Pecher, MD, Centro Manaus, Amazonas, Brazil.
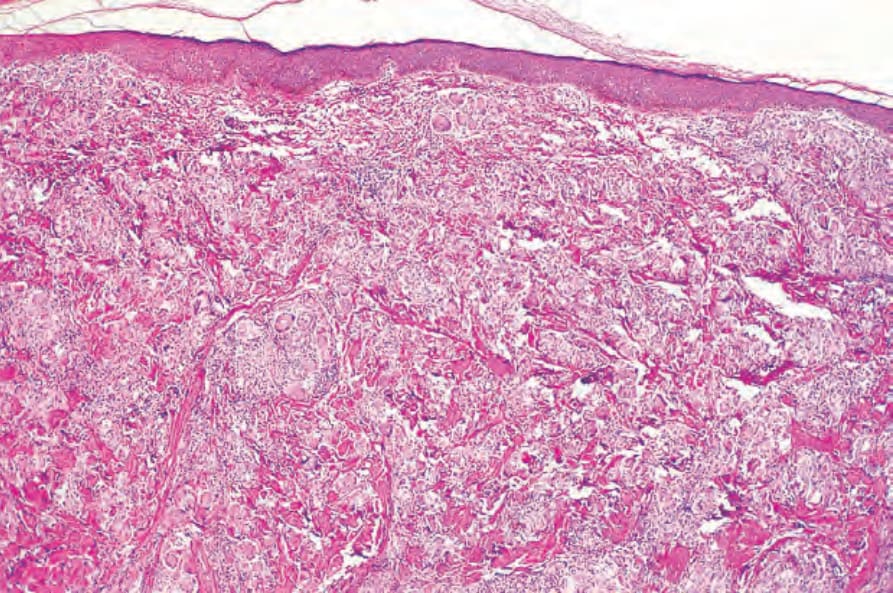
Fig. 18.375 Lobomycosis: there is an extensive granulomatous infiltrate in the dermis; the intervening eosinophilic bundles represent early keloidal scarring.
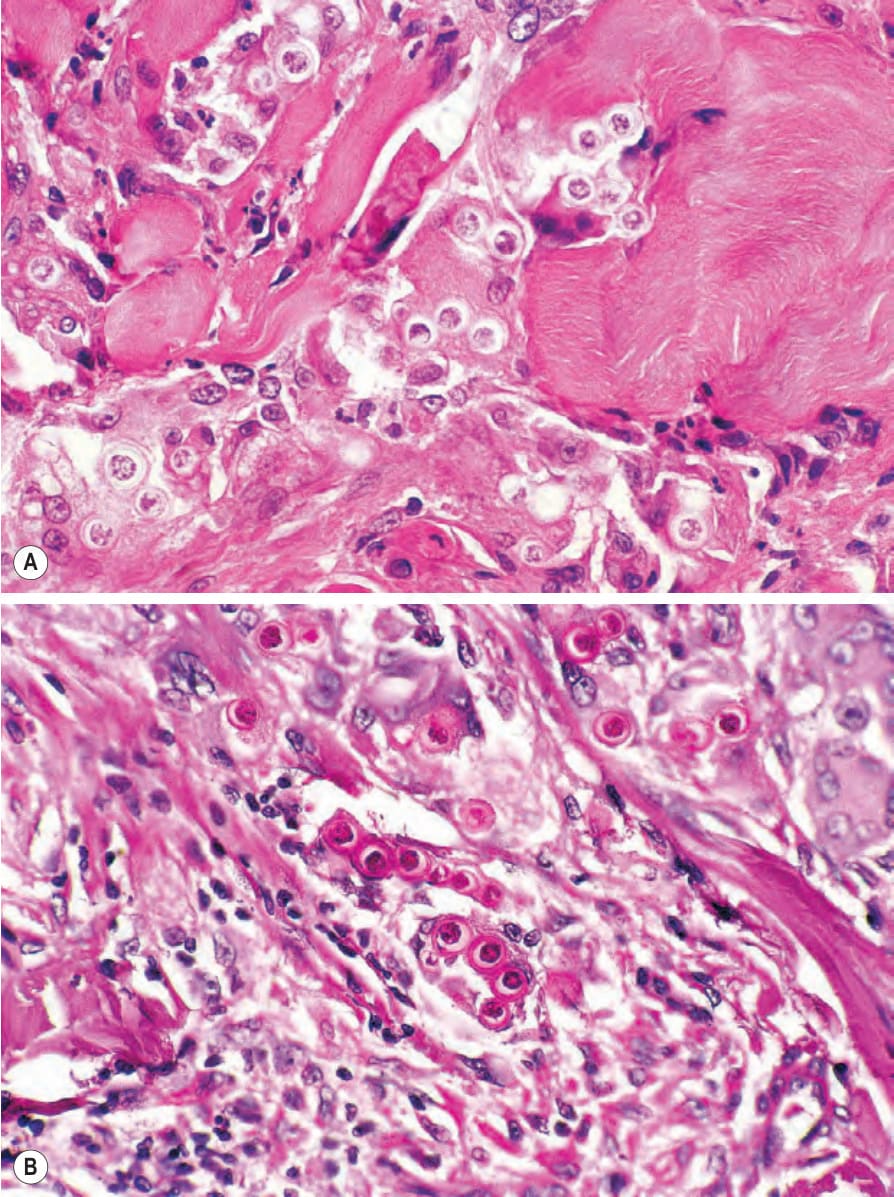
Fig. 18.376 Lobomycosis: (A) the fungi have very thick cell walls and are often arranged in chains; (B) there is striking periodic acid-Schiff positivity.