Sporotrichosis
Sporotrichosis
Clinical features Sporotrichosis is an invasive fungal infection caused by Sporothrix schenckii sensu lato, a complex comprising five species, namely, S. schenckii sensu stricto, S. globosa, S. brasiliensis, S. luriei, and S. mexicana.1–3 The organism has a worldwide distribution, although some species are geographically restricted (e.g., S. brasiliensis).2,4 It grows saprophytically in decaying vegetation and on wood.4,5 Most often it represents a localized infection limited to the skin and lymphatics, but rarely systemic disease may occur, particularly affecting the skin, bones, joints, meninges, and occasionally, the oropharyngeal region.1,6–8 It is inoculated into skin, often by wood splinters, thorns, and sphagnum moss. Rare cases have been acquired as a result of ritual tattooing.9 Man-to-man and animal-to-man transmission has also been reported, including cases transmitted by cats.4,10–13 Infection is often acquired occupationally. The condition is most common in adult males. Children, however, may also be affected.13–15 Much less often, in immunosuppressed patients, inhalation, aspiration or ingestion can result in systemic disease.5,16 Although most infections are sporadic, outbreaks of the disease have occasionally been reported.17–20 Spontaneous healing of lesions may occur.
The disease is systemic with frequent involvement of lungs, spleen, liver, lymph nodes, bone marrow, and skin.1,2,5 Patients present with fever, weight loss, anemia, cough, and skin lesions. The infection may mimic histoplasmosis clinically and radiologically.15 The skin lesions consist of erythematous papules and nodules that may appear ulcerated or show umbilication.10,12 Multiple skin abscesses may occur.16 Verrucoid skin lesions have also been described.13,17 The organism is an uncommon cause of genital ulceration.18,19 The mortality is high unless systemic treatment is given promptly. A retrospective study from Thailand revealed a mortality rate of up to 29.4%.20
Pathogenesis and histologic features T. marneffei is a thermally dimorphic fungus which produces a number of mycotoxins and other virulence factors.3,4 A presumptive diagnosis is usually possible by microscopic examination of touch preparations or tissue
961 Sporotrichosis
The cell wall components of the organism are capable of adhering to extracellular matrix proteins, in particular to fibronectin.21 This facilitates tissue invasion. In vitro experimental evidence shows that fungus is capable of adhering to and invading vascular endothelial cells. This appears to be modulated by cytokines such as TGF-β1 and could account for hematogenous dissemination of the fungus in immunocompromised patients.22,23
The cutaneous reactions to infection with Sporothrix spp. have been divided into three types: lymphocutaneous, localized (fixed) cutaneous, and disseminated cutaneous.
• In the most common form, lymphocutaneous sporotrichosis, the lesions develop at the site of inoculation (most often on exposed areas), after an incubation period of a few days to several weeks, as a nodule, which ulcerates (Fig. 18.368). Lymphatic involvement develops, with asymptomatic secondary nodules arising along the line of lymphatic drainage (Fig. 18.369). Regional lymph nodes then become enlarged. Meanwhile, the initial lesion expands as a crusted verrucous plaque.
• In the localized (fixed) form, the patient presents with pyodermatous erosions, acneiform, nodular, ulcerated, or verrucous lesions (Fig. 18.370).5,24–29 This variant may indicate a high degree of immunity.
• Disseminated cutaneous sporotrichosis is rare.30–32 There have, however, been a number of reports of this form of disease in patients with HIV/ AIDS.33–36 Sporotrichosis is an uncommon cutaneous manifestation of IRIS in HIV-infected patients who have received ART.37,38
The extracutaneous forms, which include pulmonary and systemic variants, are very rare.1,15,39 Visceral involvement may occur in the absence of cutaneous lesions. Primary pulmonary infection and disseminated systemic sporotrichosis is seen in the immunosuppressed and occurs most often in alcoholics and patients with pulmonary tuberculosis, sarcoidosis, diabetes mellitus, and chronic steroid treatment.5 This form of the disease has also been reported as an emerging mycosis in patients with HIV infection.16
Histologic features S. schenckii sensu lato is a thermally dimorphic fungus which is filamentous in culture but yeast-like in tissues.40 The organism is not easily seen with conventional staining and is best demonstrated with methenamine silver or PAS stains. It presents as round to oval bodies, 4–6 µm in diameter, sometimes within giant cells. Occasionally, the spores are seen as thin cigar-shaped rods up to 8 µm long; rarely, these may be present in conspicuous numbers.5,16,27 They may be present in the center of eosinophilic radiating material, an example of the Splendore-Hoeppli phenomenon (Fig. 18.371).41 This structure represents an immunological reaction between host and fungus. Indirect immunofluorescence has revealed that a portion thereof comprises antigenically related IgG and IgM molecules.42 These so-called
962 Infectious diseases of the skin
A
asteroid bodies are characteristically located within intradermal microabscesses, and suppurative granulomas in particular (Fig. 18.372).43,44 Examination of many serial sections is often required for identification of these elusive structures. Occasionally, hyphae may be identified in PAS-stained sections. The mycelial form of the organism (including conidia) may also be observed in the dried-up purulent exudate in chronic ulcerated lesions.45 Surrounding the giant cells containing the often scanty organisms is an intense granulomatous infiltrate. Lymphocytes, plasma cells, and histiocytes are also present. The overlying epidermis shows acanthosis with areas of pseudoepitheliomatous hyperplasia; ulceration is often evident. Neutrophil abscesses are present in both acanthotic epidermis and dermis.16,46
The nodules resulting from lymphatic spread are located in the deep dermis or subcutaneous tissues. They consist of a central necrotic zone with neutrophils, a surrounding zone of epithelioid cells and giant cells, and an outer zone of plasma cells and lymphocytes with fibrosis.5,41
B
Although the tissue reaction is often suggestive of sporotrichosis, confirmation should be sought by isolation and culture of the organism. The organism may also be demonstrated by immunohistochemistry.16,47 Infection can also be confirmed by PCR.16,48

Fig. 18.368 Sporotrichosis: note the multiple nodules with ulceration on the shin, which is a characteristic site. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.

Fig. 18.369 Sporotrichosis: multiple nodules are present along the lymphatic channels draining the primary lesion. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.

Fig. 18.370 Sporotrichosis: localized variant presenting as an ulcerated plaque. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu- Natal, South Africa.
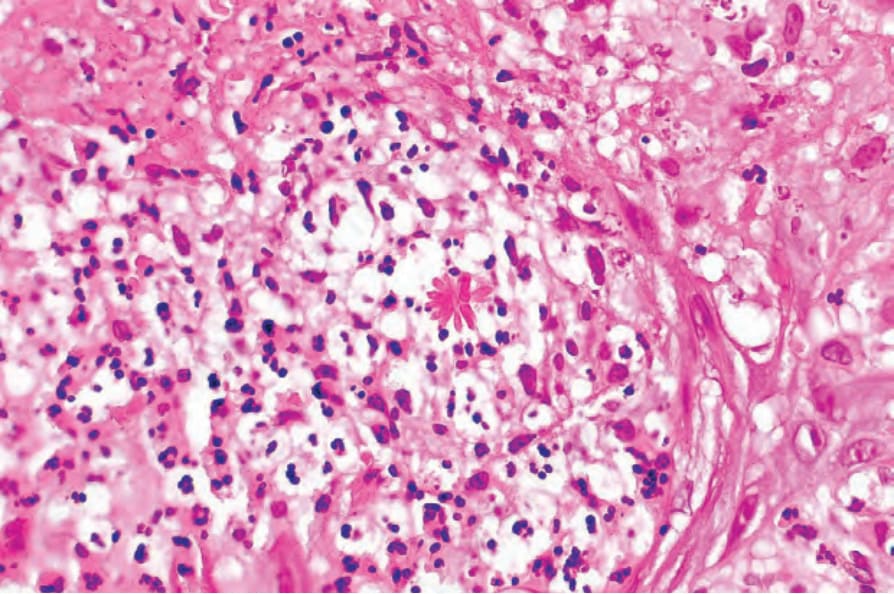
Fig. 18.371 Sporotrichosis: the yeast form is characteristically surrounded by radiating eosinophilic spokes (the Splendore-Hoeppli phenomenon).
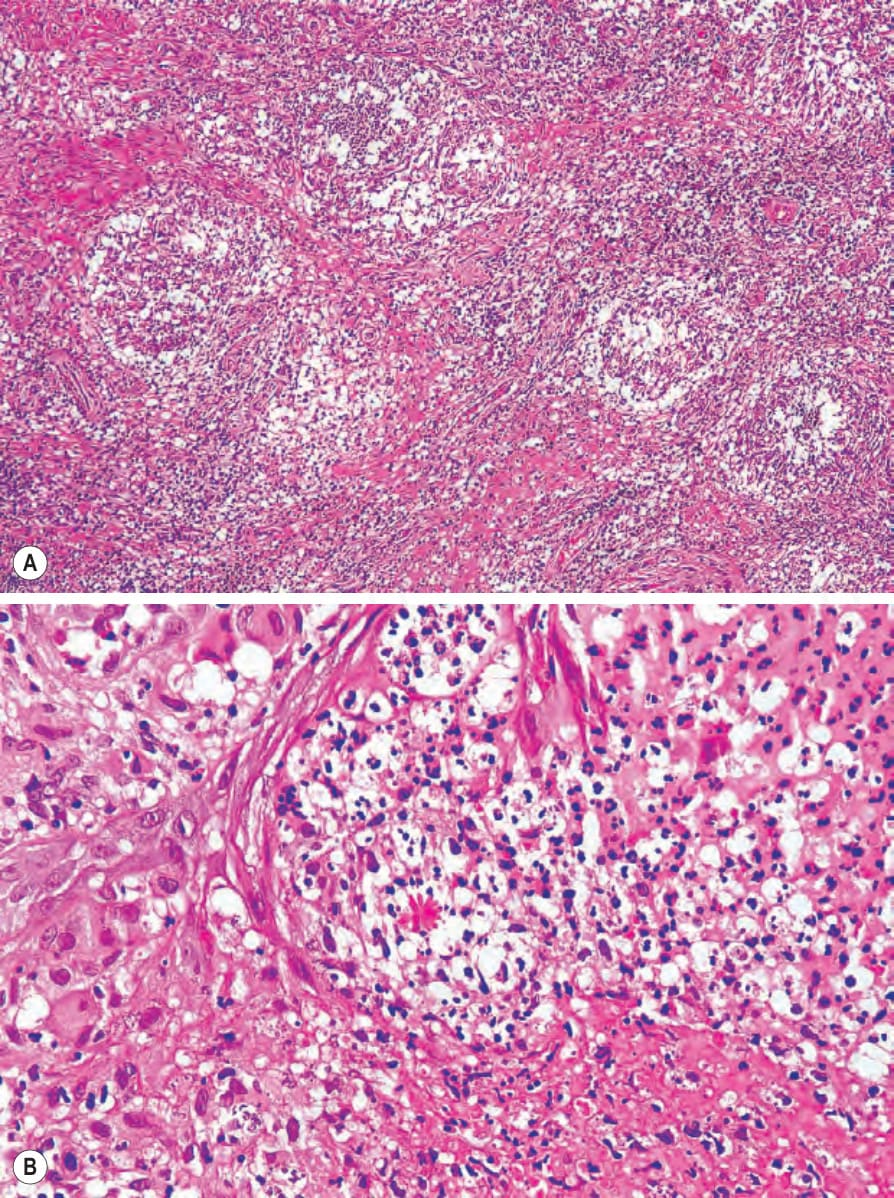
Fig. 18.372 (A, B) Sporotrichosis: multiple dermal abscesses are typically present in this condition.