Penicilliosis
Penicilliosis
obtained by aspiration and stained with Wright.6,7 Histologically, a granulomatous response is usually minimal or absent. Instead, there is focal necrosis and a predominantly perivascular inflammatory cell infiltrate consisting of scattered neutrophils with nuclear dust, lymphocytes, and variable numbers of histiocytes. Necrosis is particularly prominent in immunocompromised patients. Organisms are abundant and present in the cytoplasm of histiocytes (Fig. 18.367). Extracellular organisms are also seen, often singly. Oval and elongated yeasts are identified on staining with PAS and Grocott. Their diameters range from 2 to 8 µm.21,22 The small yeasts do not bud but instead divide by fission; the resultant appearance is said to be reminiscent of a sausage with a transverse septum, with the latter appearing thicker than the wall of the yeast.22 In addition to culture, PCR may be employed to confirm the diagnosis.21,23
Clinical features Penicilliosis is caused by Talaromyces marneffei (formerly Penicillium marneffei), an organism that was first discovered in the bamboo rat (Rhizomys sinensis) in the 1950s.1–4 The fungus is endemic in countries of Southeast Asia, particularly Thailand, and also in the south of China.3,5,6 The fungus also occurs in northeastern India.7 The organism has become an important cause of morbidity and mortality in patients infected with HIV. The great majority of patients with penicilliosis are HIV positive, and the infection is an important AIDS-defining condition in the aforementioned endemic areas.3,8 HIV infected patients who have traveled to or lived in Southeast Asia, however, may present with the disease following their return to nonendemic countries.8,9 Penicilliosis has also emerged as a potential manifestation of IRIS among those receiving ART.10–13 Not all patients with T. marneffei infection, however, are HIV-infected adults; the disease has even been documented in HIV-negative infants on rare occasions.14
Differential diagnosis Distinction from leishmaniasis is based on the presence of a kinetoplast in the latter. Distinction from histoplasmosis is based on the fact that H. capsulatum displays narrow-necked budding while T. marneffei divides by fission, with visible septation. Although there are obvious geographic differences, penicilliosis should also be distinguished from emmonsiosis, given the clinical and morphological similarities between the latter and histoplasmosis.
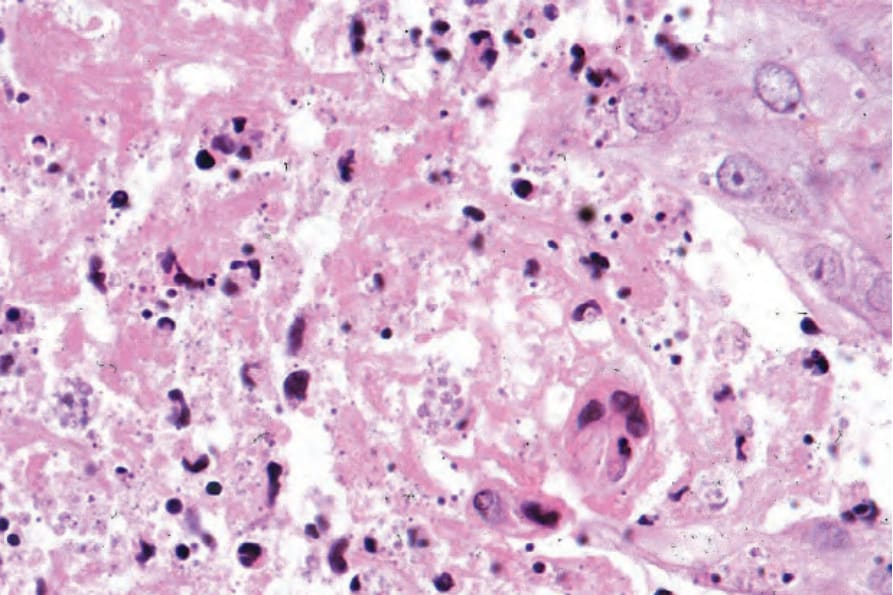
Fig. 18.367 Penicilliosis: numerous organisms are present within the cytoplasm of histiocytes.