Emmonsiosis
Emmonsiosis
Clinical features Disseminated infection with what was initially regarded as a novel species of Emmonsia, was described recently among South African patients with HIV/ AIDS, almost all of whom had skin lesions at presentation.1–5 Although the causative agent was briefly assigned the name Emmonsia africanus, it has since been named Emergomyces africanus.6,7 ART had been initiated within the preceding 2 months in 24% of the HIV co-infected patients, thereby suggesting the presence of unmasking IRIS.1,2 Immunocompetent individuals are only rarely affected.2,4,5 Prior to 2013, there was no known association between Emmonsia/Emergomyces infection and HIV/AIDS in sub-Saharan Africa.5 There is, however, a strong likelihood that a significant number of cases of emmonsiosis might have been misclassified as histoplasmosis in the past. Furthermore, Emmonsia spp. and Emergomyces spp. display phylogenetic proximity to Histoplasma spp. and other organisms in the family Ajellomycetaceae.3,5–7
Emergomyces africanus is a novel thermally dimorphic pathogenic fungus, which on initial molecular phylogenetic analysis was found to be most closely related to Emmonsia pasteuriana. The latter is an organism with an as yet unidentified environmental or animal source, and was recently renamed Emergomyces pasteurianus.1,7 Emergomyces pasteurianus is a rare cause of disseminated disease in immunocompromised hosts, with only isolated cases recorded to date, including a transplant recipient in Spain with HIV co-infection, an ART-naïve Italian female with AIDS, a German farmer on long-term corticosteroid therapy who developed progressive pneumonic illness, a Chinese transplant recipient, and a South African patient with
Pathogenesis and histologic features The histologic appearances of Emergomyces africanus infection are virtually indistinguishable from histoplasmosis in most cases. Skin biopsies reveal a granulomatous and/or suppurative dermal infiltrate in response to variable numbers of small globose or oval fungal yeasts, with single or multiple narrow-based budding.1,2 In some cases, the host inflammatory response is minimal, with large numbers of extracellular and intracellular organisms visible (Fig. 18.366). The latter are present within macrophages. PAS and
960 Infectious diseases of the skin
silver stains highlight the yeast morphology and are helpful in declaring the fungi in those cases where organisms are relatively sparse. The yeasts measure 2–7 µm in diameter.2 Cases occurring as a manifestation of IRIS are said to exhibit a more pronounced mixed dermal inflammatory infiltrate, and even microabscess formation.1,2 Skin biopsy allows for relatively rapid diagnosis, with confirmation thereof by means of pan-fungal PCR. The aforementioned technique targets the nuclear ribosomal internal transcribed spacer region and may facilitate both rapid speciation as well as distinction from other thermally dimorphic fungi.5–7,16
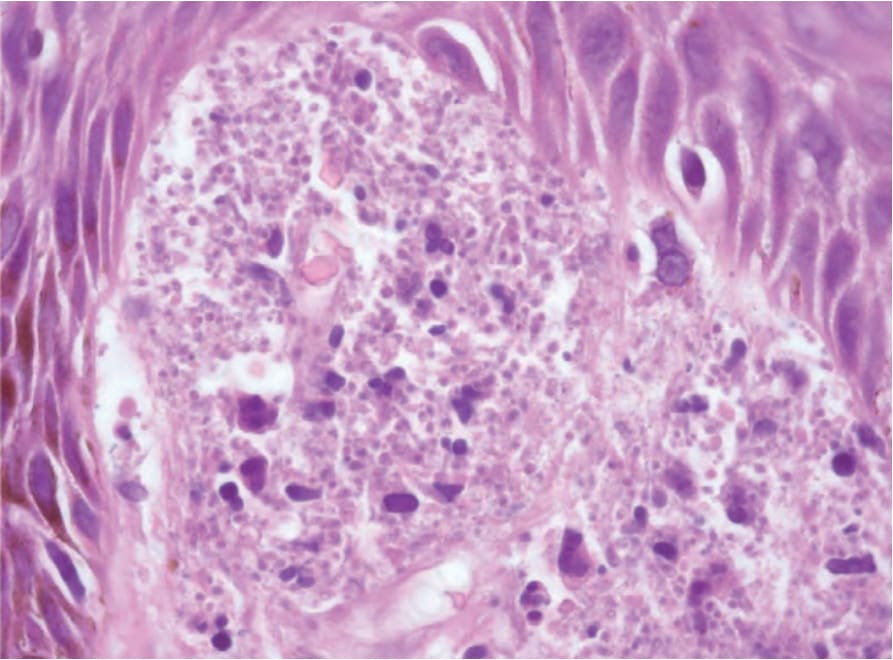
Fig. 18.366 Emmonsiosis: considerable numbers of small intracellular and extracellular yeasts are present.
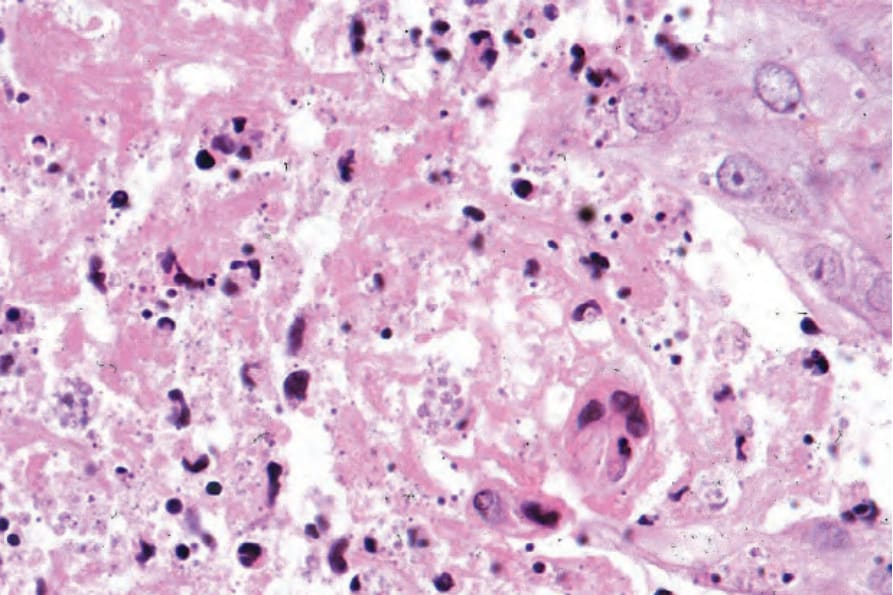
Fig. 18.367 Penicilliosis: numerous organisms are present within the cytoplasm of histiocytes.