Histoplasmosis
Histoplasmosis
Clinical features Histoplasmosis is caused by two very similar fungi, Histoplasma capsulatum var. capsulatum (H. capsulatum) and the African clade of H. capsulatum (formerly referred to as H. capsulatum var. duboisii). Despite the
957 Histoplasmosis
Chronic pulmonary (cavitatory) histoplasmosis (buckshot calcification) and disseminated disease are also recognized variants.1,2,8 Chronic pulmonary histoplasmosis may sometimes mimic secondary tuberculosis. Disseminated histoplasmosis is uncommon, but may rarely occur in immunocompetent hosts.9,10 It is, however, an important complication of immunosuppression including that seen in HIV/AIDS.1,10–17 Lesions are particularly seen in the liver, spleen, lymph nodes, and bone marrow.7 A wide variety of systems may be involved, however, and therefore symptoms and signs are very variable. Fever and weight loss, although non-specific, are common.12,14,15
A
Disseminated histoplasmosis may be classified into acute, subacute, and chronic forms in diminishing degrees of severity.8,9 The acute form usually affects infants while chronic disseminated histoplasmosis is characteristically seen in adults. Patients with HIV/AIDS are at particular risk of developing lethal progressive disseminated histoplasmosis.2,16 Under such conditions, it has been suggested that the disease may sometimes represent reactivation of a quiescent lesion.7,8 The possibility of patient-to-patient transmission has also been reported.18 In patients with HIV/AIDS-associated disseminated histoplasmosis, a combination of antifungal therapy and ART may result in a dramatic improvement in clinical outcome.19 Histoplasmosis is also a potential manifestation of IRIS among HIV-infected individuals receiving ART.20 Disseminated histoplasmosis can occasionally be the initial mode of presentation of an HIV infection.12
Cutaneous involvement is uncommon and is almost always a feature of disseminated (fungemic) disease. It is said to occur in 4% to 11% of cases in general, but is encountered in 10% to 25% of AIDS-related cases.8,11,21,22 An Indian study of 37 cases of disseminated histoplamosis revealed a much higher frequency of skin involvement among immunocompromised patients than immunocompetent subjects (54.5% and 11.5%, respectively).10 Lesions are most common on the arms, face, and trunk, but obviously may be encountered elsewhere.12 Skin lesions present as macules, papules, nodules, pustules, indurated (sometimes ulcerated or verrucous) plaques, purpura, pyoderma gangrenosum-like lesions, abscesses, furuncles, cellulitis, eczematous eruptions, acneiform eruptions, MC-like lesions, punched-out ulcers, panniculitis, and subcutaneous nodules.7,22–27 Oral ulcers may also be present.12,14,26 An unusual case with vaginal ulcerations as the presenting sign of disseminated infection has been reported.28 There have also been rare reports of penile ulceration in this clinical context.29 Diffuse cutaneous hyperpigmentation sometimes reflects an underlying histoplasmosis-related Addison disease.12 Erythema nodosum and erythema multiforme are not infrequent hypersensitivity manifestations.7,30
B
The very rare primary cutaneous lesions (representing local inoculation) present as nodules, ulcers, cellulitis, or lymphangitis.7,31
African clade of Histoplasma capsulatum (H. capsulatum var. duboisii) For convenience, use of the historic designation H. capsulatum var. duboisii will be retained in this section. This organism usually occurs in equatorial Africa although it has been documented elsewhere on rare occasions.32–34 Occasional cases have been encountered in Europe, reflecting the impact of travel and immigration patterns.4 It has two main forms of presentation:
• Patients may develop a localized chronic form with single lesions in the skin, subcutaneous fat, or bone.
• Patients may manifest disseminated disease, which in addition affects lymph nodes and abdominal viscera.2
morphological similarity, the two species have different geographical distributions and clinical presentations (Fig. 18.359).1
Histoplasma capsulatum H. capsulatum is very common in North America (Ohio and Mississippi river valleys) but is seen worldwide.1,2 Around 105 outbreaks of histoplasmosis occurred in the United States and Puerto Rico between 1938 and 2013, and involved some 2850 cases.3 It is rare in Europe, although cases have occurred there since the advent of the HIV/AIDS pandemic.4,5 It is present in soil and in poultry and bat droppings, and the infection has also been reported following the chopping of rotten wood and the renovation or demolition of old buildings.1,6 Spore inhalation can cause an acute pulmonary infection (if the inoculum is very large), but it is probable that more often a subclinical infection provokes a positive histoplasmosis skin test.7
Skin lesions include superficial cutaneous and subcutaneous granulomata and abscesses and osteomyelitis with overlying cutaneous spread.6,35 The calvarium and long bones are predominantly affected.6 In contrast to H. capsulatum, pulmonary disease is rare. Furthermore, patients are usually not immunocompromised.34,36,37
Pathogenesis and histologic features H. capsulatum is a dimorphic fungus appearing as a mycelium at room temperature, but growing as a yeast at body temperature.2 Despite its name, it is not encapsulated. Infection is most commonly transmitted by the inhalation of spores or hyphae of H. capsulatum. The hyphal form grows in the soil; the yeast form (2–4 µm in diameter) occurs in the tissues, entirely intracellularly following inhalation of the spores.
958 Infectious diseases of the skin
The tissue response to infection with H. capsulatum parallels that seen with Mycobacterium tuberculosis including primary lesions, reinfection, and the development of caseation.7 Following pulmonary and nodal involvement, susceptible people develop a fungemia, with spread of the organism widely throughout the body. A chronic tuberculoid granulomatous inflammatory response develops. The yeast is present within distended macrophages as a basophilic dot with a surrounding artifactual halo (pseudocapsule) (Fig. 18.360).1 Its features are similar to those of Leishmania, but it lacks the kinetoplast. It may be further differentiated by the use of special stains including the PAS reaction and methenamine silver (Fig. 18.361).35 Transepidermal elimination of Histoplasma has been reported in association with HIV/AIDS.23,38 It should be noted that some HIV/AIDS-associated cases lack a granulomatous tissue response and may instead show focal necrosis and a mild perivascular and interstitial infiltrate with predominantly polymorphonuclear leukocytes, lymphocytes, and some histiocytes. Karyorrhexis may be a prominent feature, resulting in potential confusion with atypical leukocytoclastic vasculitis.39 Involvement of cutaneous nerves by the organism has also been described in association with HIV/AIDS.40 Biopsies from profoundly immunosuppressed individuals may reveal a negligible or absent host response to these organisms.41
H. capsulatum var. duboisii is also seen intracellularly, but usually within multinucleate giant cells (Figs 18.362–18.364). It is a large yeast, 7–15 µm in diameter, with characteristically thick cell walls.1 Narrow-based budding may be seen and short chains are occasionally formed.2 The early stages are followed by necrosis and then by a granulomatous and fibrous reaction.
Differential diagnosis Emmonsiosis, a disseminated HIV/AIDS-related fungal infection caused by Emergomyces africanus, is almost indistinguishable from histoplasmosis. It is likely that rather than being a true emerging pathogen in South Africa (where the organism was recently identified), many cases diagnosed as H. capsulatum infection solely on morphological grounds in the past were, in fact, examples of Emergomyces infection. The yeasts measure 2–7 µm in diameter, and may be intracellular and/or extracellular.42,43 This condition is discussed elsewhere in this chapter.
H. capsulatum var. capsulatum must also be differentiated from Penicillium species, especially since both infections share clinical and radiological features.44 Macrophages parasitize both organisms. H. capsulatum is characterized by narrow-necked budding while Penicillium divides by
959 Emmonsiosis
septation. Microforms of Blastomyces dermatitidis, capsule-deficient forms of Cryptococcus neoformans, and endospores of Coccidioides spp. are additional sources of potential diagnostic confusion.1,35 Although fungal culture remains the gold standard for diagnostic confirmation, and an in situ hybridization-based technique for use on paraffin-embedded material that enables distinction from other invasive fungal pathogens has been described, newer pan-fungal PCR techniques targeting the nuclear ribosomal internal transcribed spacer region hold promise in facilitating more rapid and precise speciation on formalin-fixed biopsy material.42,43,45
Skin involvement by histoplasmosis should also not be confused with CL (see above). Although the intracellular Leishmania organisms contained within macrophages resemble the yeasts of H. capsulatum, the former possess a kinetoplast and stain with the Giemsa method.
H. capsulatum var. duboisii may be distinguished from B. dermatitidis by having single rather than multiple nuclei.
AIDS.1,2,7–11 The inhaled conidia of both Emergomyces spp. possess the capacity for conversion to a yeast phase in mammalian tissue, with subsequent extrapulmonary dissemination.1,2 This is in contrast to Emmonsia parva and Emmonsia crescens, the causative agents of adiaspiromycosis. The latter is a chronic granulomatous lung disease of rodents and occasionally humans, and is characterized by the transformation of inhaled conidia into large adiaspores measuring 50–500 µm in diameter.2,12–15
Skin lesions are an almost universal finding among HIV/AIDS patients with disseminated emmonsiosis caused by Emergomyces africanus. The spectrum of cutaneous involvement is protean, with skin lesions potentially misdiagnosed clinically as varicella, secondary syphilis, seborrheic dermatitis, guttate psoriasis, disseminated cutaneous tuberculosis, Kaposi sarcoma, pyoderma gangrenosum, or even an adverse drug reaction.2 Patients may present with erythematous and sometimes scaly, hyperpigmented or verrucous papules and plaques, ulcers, or crusted, boggy plaques (Fig. 18.365).1,2,5 Penile, lip or palatal mucosal lesions have also been described. Rare skin lesions may exhibit central umbilication.1,2 Lower respiratory tract involvement is seen in almost all cases, with chest radiographs revealing diffuse or focal infiltrates, lobular atelectasis, and/or hilar lymphadenopathy. Upper respiratory tract involvement may also occur, manifesting with epistaxis, congestion, non-specific symptoms, or even oroantral fistula formation. Although neurological symptoms are common, no organisms could be isolated from the cerebrospinal fluid of affected individuals in the largest series reported to date.2 Blood and bone marrow involvement are common.1,2 Disseminated emmonsiosis carries a mortality of up to 48%, and the condition is uniformly fatal if left untreated.2 Concurrent opportunistic co-infections are not uncommon.2,5 The detection of Histoplasma antigen in the urine is a potentially useful diagnostic adjunct, given the apparent cross-reactivity with Emergomyces (Emmonsia) spp.2

Fig. 18.359 Histoplasma capsulatum: (A) note the ulcerated lesions on the scrotum and thigh. This patient was HIV positive; (B) duboisii variant showing innumerable disfiguring papules, nodules, and plaques. (A) By courtesy of C. Furlonge, MD, Port of Spain, Trinidad; (B) by courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.
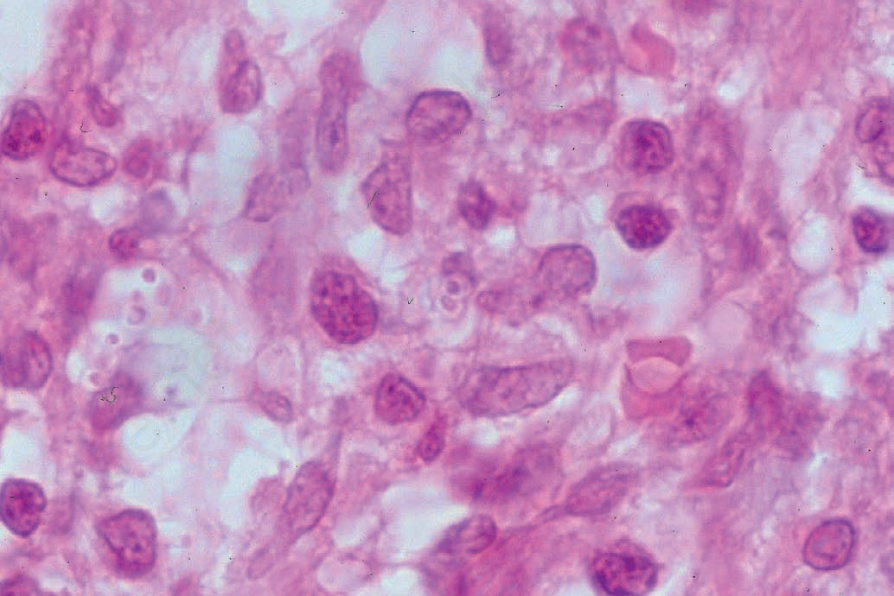
Fig. 18.360 Histoplasma capsulatum: the small yeast forms are intracellular and consist of a small basophilic particle surrounded by a clear halo (a cytoplasmic retraction artifact). By courtesy of R. Carr, MD, Warwick Hospital, Warwick, UK.
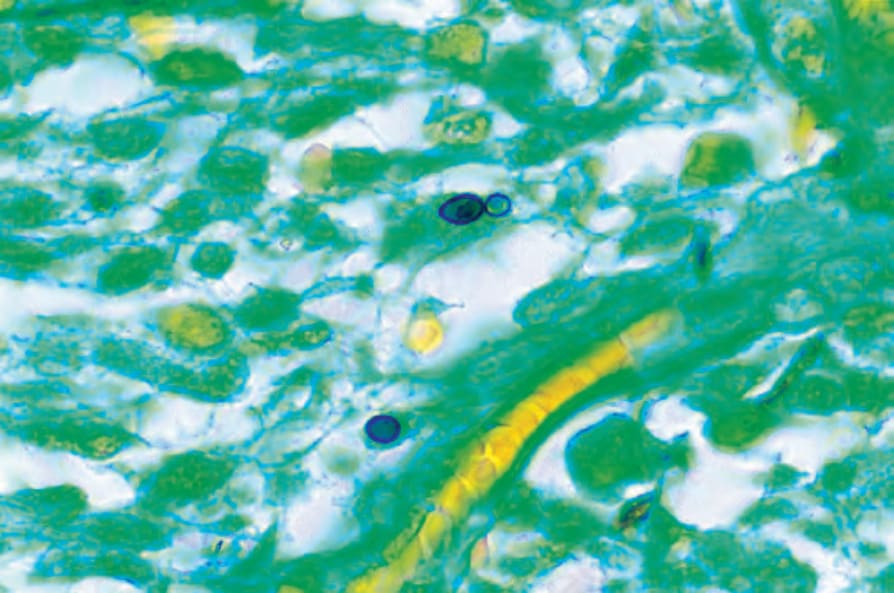
Fig. 18.361 Histoplasma capsulatum: differentiation from leishmaniasis is readily effected by the use of methenamine silver. By courtesy of R. Carr, MD, Warwick Hospital, Warwick, UK.
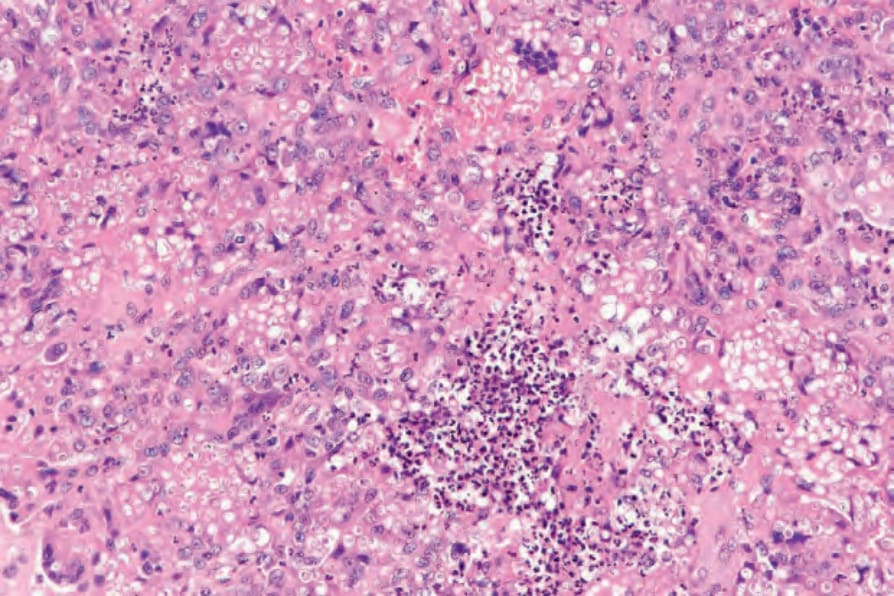
Fig. 18.362 Histoplasma duboisii: a dense granulomatous infiltrate is present in the reticular dermis. The organisms are larger than Histoplasma capsulatum and are located within giant cells. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.
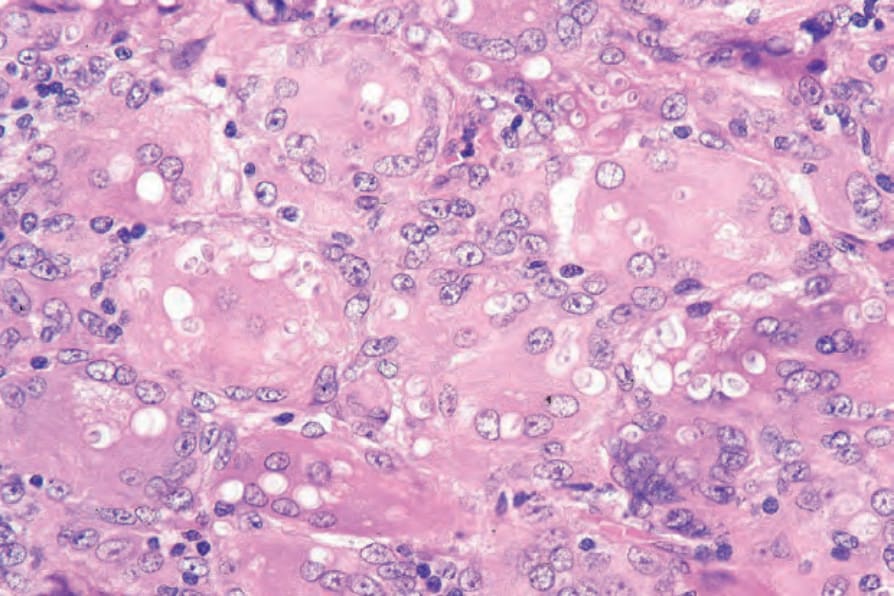
Fig. 18.363 Histoplasma duboisii: the yeast cells have very thick walls and the nuclei are single. This distinguishes Histoplasma duboisii from Blastomyces dermatitidis, in which nuclei are multiple. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.

Fig. 18.364 Histoplasma duboisii: the fungi are highlighted with the methenamine silver stain. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.

Fig. 18.365 Emmonsiosis: widespread crusted papules and plaques in a patient with underlying AIDS. By courtesy of M. Ruhani, MD, Division of Dermatology, University of the Witwatersrand, Johannesburg, South Africa.