Pheohyphomycosis
Pheohyphomycosis
Clinical features
Phaeohyphomycetes are a heterogeneous group of pigmented (dematiaceous) fungi with both yeast-like and hyphae-like forms in tissues.1–4 The sclerotic bodies of chromoblastomycosis are not seen. There are > 100 known causative species, all of which show pigmented yeast-like cells, pseudohyphae, and distorted short or long hyphae in variable proportions.2,5
Pheohyphomycosis can be subdivided into superficial, cutaneous, corneal, subcutaneous, and systemic/disseminated forms.4–8 Keratitis, otomycosis, tinea nigra palmaris, and rare infections of the ungual apparatus are additional manifestations.8–10
• Black piedra caused by P. hortae is an example of superficial pheohyphomycosis affecting the hair shaft.6,11
• Cutaneous lesions include macules, papules, plaques, nodules, cystic or verrucous lesions, sometimes with ulceration.4,12–14 A cystic lesion is referred to as a pheohyphomycotic cyst; the latter may also be subcutaneous in location.15
C
• Exophiala jeanselmei is the most common cause of subcutaneous pheohyphomycosis, the patients presenting with a solitary discrete asymptomatic well-circumscribed subcutaneous nodule.5,16 These usually follow trauma, most often to the limbs.4,17 E. jeanselmei is also an important cause of cutaneous pheohyphomycosis.18 Other documented etiological agents in subcutaneous pheohyphomycosis include Fonsecaea pedrosoi, Phaeoacremonium spp., Cladophialophora spp., Chaetomium
955 Pheohyphomycosis
globosum, E. spinifera, E. salmonis, E. oligosperma, Lasiodiplodia theobromae, Phialophora spp., Coniothyrium spp., Cladosporium spp, Wallemia sebi, and Pyrenochaeata romeroi.15,19–34
Pheohyphomycosis may also present in the immunosuppressed, especially those who have received organ transplants.1,35,36 Patients receiving long-term oral corticosteroids are also at risk.18 Nodules often become large (up to several centimeters across), but epidermal involvement is not seen. The necrotic yellow-gray central contents can be aspirated from well-developed lesions.
Disseminated (systemic) pheohyphomycosis carries a mortality of almost 80%.2,5 The organism most frequently implicated is Scedosporium prolificans, and although some patients have been immunocompetent, the majority of infections have occurred in immunocompromised individuals.2,4,7 Endocarditis may occur, particularly in relation to prosthetic cardiac valves. Organisms implicated less frequently are Bipolaris spicifera and Wangiella dermatitidis.2 A case of disseminated pheohyphomycosis caused by Ochronocis gallopavum has been reported in a marijuana user with advanced HIV infection.37
Infection with Alternaria spp. (alternariosis) is discussed elsewhere.
Pathogenesis and histologic features Phaeohyphomycetes are present in vegetation, soil, and decaying organic material.2 The disease occurs by traumatic implantation. Phaeohyphomycetes are mostly opportunistic pathogens.4 Virulence factors include melanin and enzymes such as proteases, peptidases and hyaluronidases.1,2,8,38
E. jeanselmei is seen as yellow-brown/chestnut-brown, irregularly swollen, septate hyphae, which can be branched or unbranched.5 Yeast-like forms are also seen, sometimes in chains.1 The organisms occur in the necrotic center of the abscess and in the surrounding cellular infiltrate of epithelioid macrophages, giant cells, and neutrophils (Figs 18.353–18.355).4,19 Sometimes, it can be very difficult to find the organisms, and special stains such as PAS or methenamine silver can be invaluable (Fig. 18.356).38 A wood splinter may occasionally be present. There is a dense fibrotic reaction around the inflammatory component.5
Fungal culture and/or PCR studies are required for precise identification of the etiological species.
Differential diagnosis Pheohyphomycosis is distinguished from chromoblastomycosis by the absence of the pigmented sclerotic bodies seen in tissue sections in the latter condition. It is of interest that the same fungus may cause either condition depending on the response to the host’s internal environment.3,4,17 Pigment is sometimes not readily apparent within the fungal walls on H&E staining, resulting in potential confusion with hyaline septate fungi
956 Infectious diseases of the skin
A
B
(hyalohyphomycosis). In such cases, a Masson-Fontana stain is a useful means of highlighting the melanin.19,38
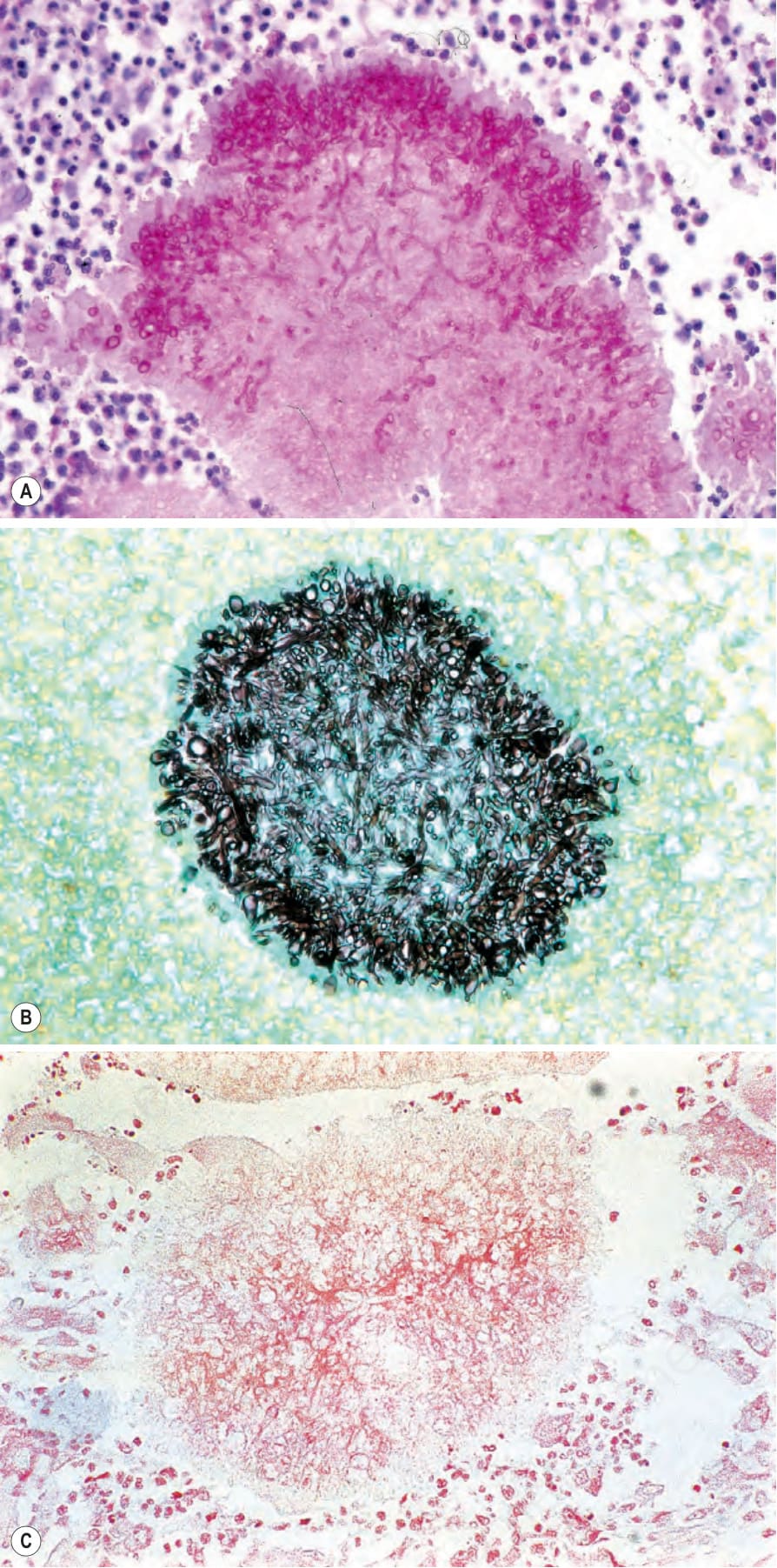
Fig. 18.351 (A–C) Mycetoma: the use of special stains readily confirms the fungal nature of this variant. (A) Periodic acid-Schiff; (B) methenamine silver; (C) Gram.
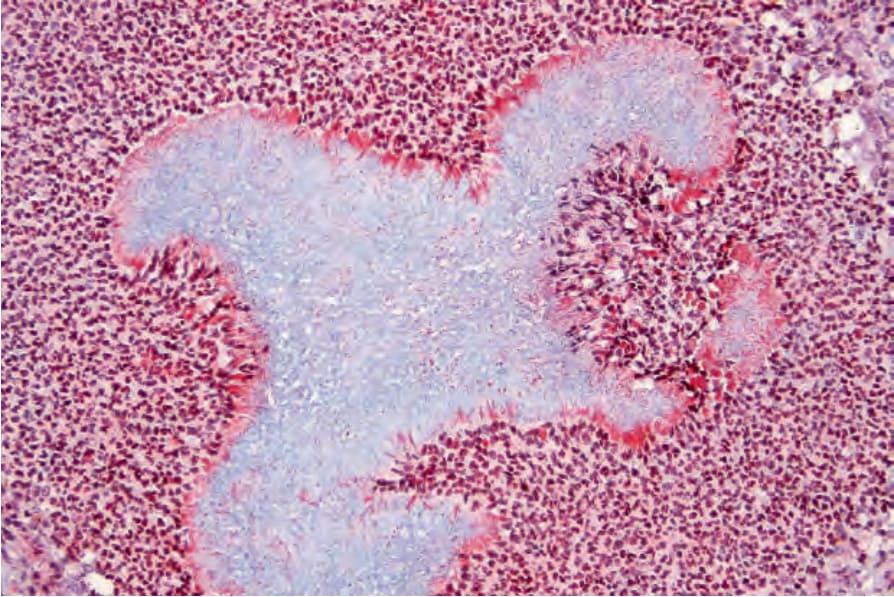
Fig. 18.352 Mycetoma: this fibrin stain highlights the Splendore-Hoeppli phenomenon.
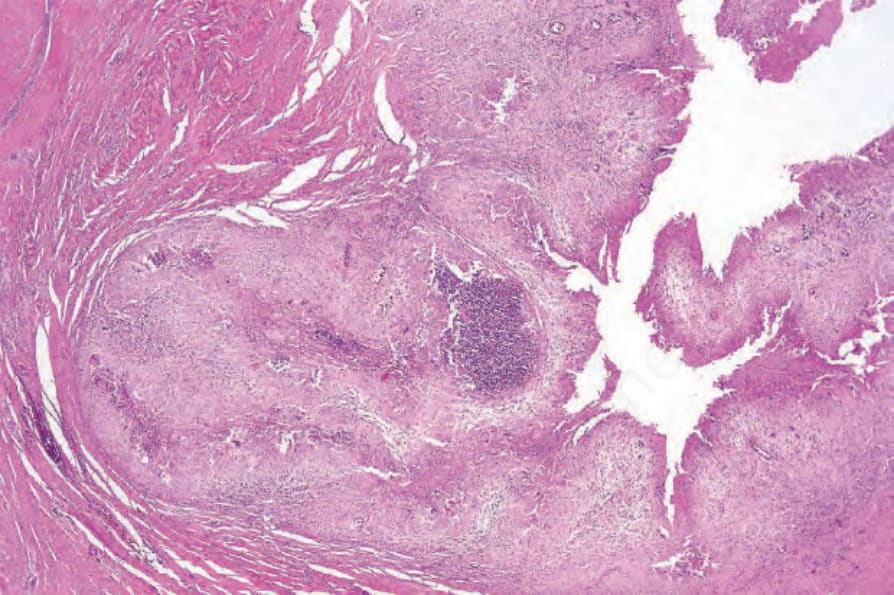
Fig. 18.353 Pheohyphomycosis: this low-power view shows the typical appearance of a deep dermal discrete nodule.
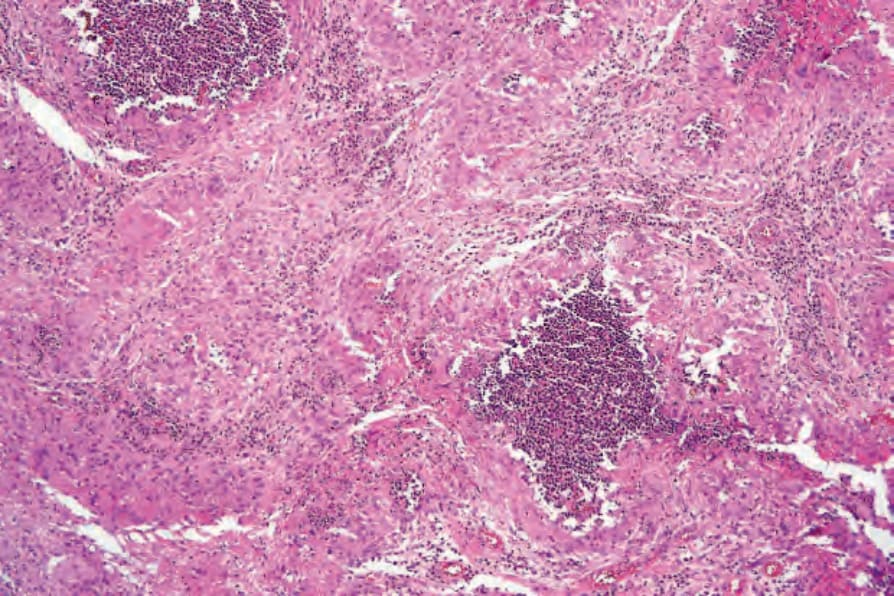
Fig. 18.354 Pheohyphomycosis: higher-power view showing mixed suppurative and granulomatous inflammation.
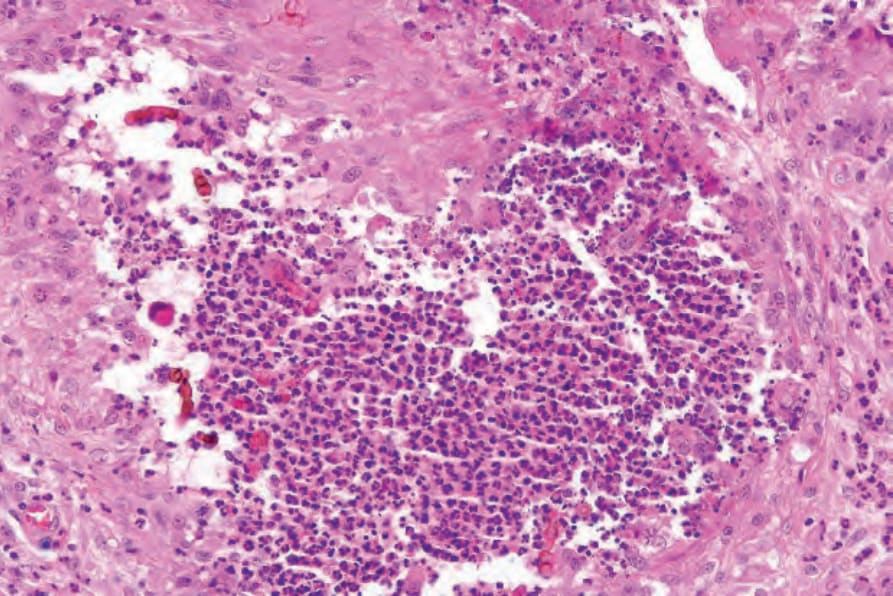
Fig. 18.355 Pheohyphomycosis: pigmented yeast forms, some forming in chains, are present.
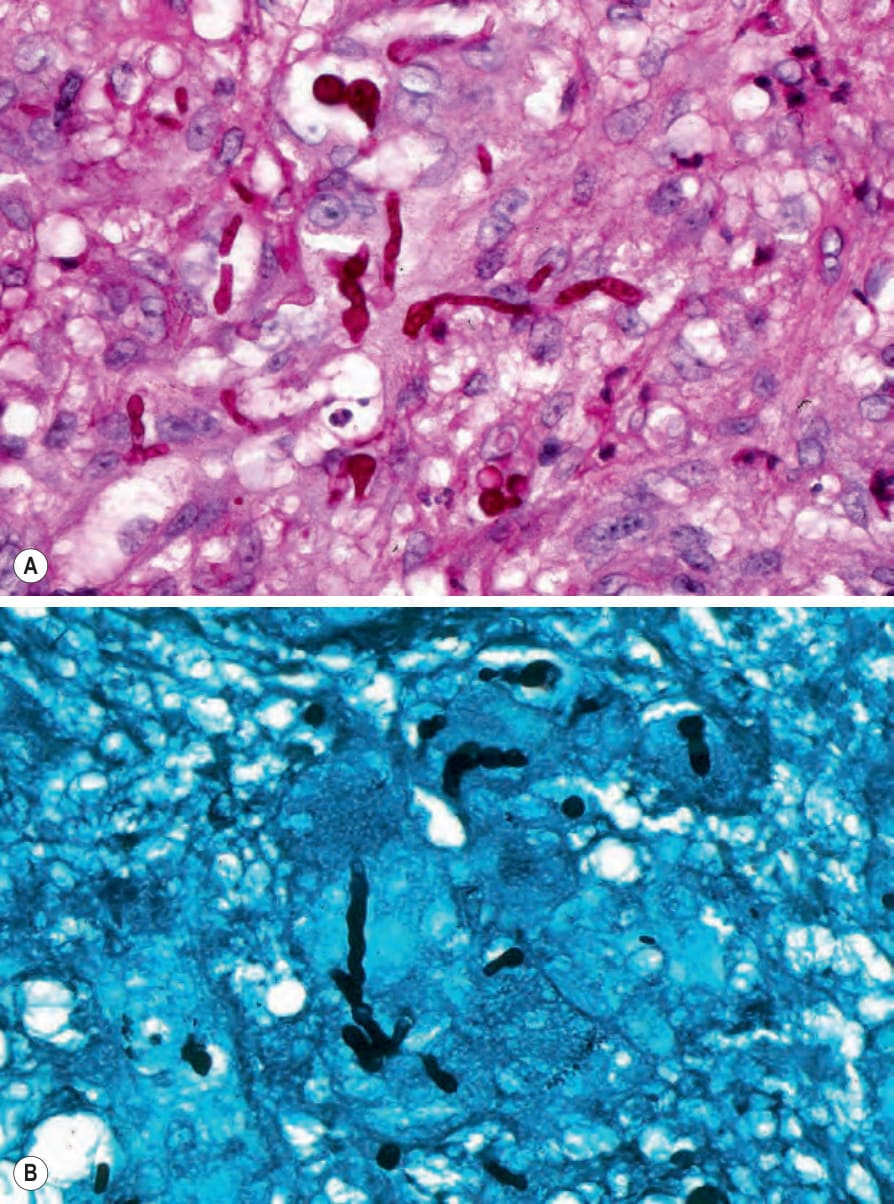
Fig. 18.356 Pheohyphomycosis: the hyphae can be highlighted with (A) periodic acid-Schiff and (B) silver stains.

Fig. 18.357 Cutaneous alternariosis: crusted ulcer at the base of the thumb. By courtesy of S.W. Lanigan, MD, Bridgend General Hospital, Bridgend, UK.