Mycetoma
Mycetoma
Clinical features Mycetoma (Gr. mykes, fungus; oma, tumor) is a chronically discharging infection of skin and subcutaneous tissue, characterized by multiple sinus tracks and the presence of granules in the exudate.1–7 It can be caused by bacteria (actinomycetoma) (e.g., Nocardia, see above) or (less commonly) by fungi (eumycetoma). Mycetoma is more or less confined to tropical zones, mainly between the latitudes of 15° South and 30° North (the so-called ‘mycetoma belt’).5,8 The disease most commonly occurs on the foot, although other sites can be affected (Fig. 18.345).
Repeated inoculation by minor trauma is necessary to produce a lesion, which begins as a papule and enlarges to become a discharging nodule. This process extends to the adjacent skin and the discharging fistulae do not heal (Fig. 18.346). The affected area becomes distorted by inflammation and fibrosis, and the underlying bone may become involved. Mycetoma occurs most commonly in 20- to 50-year-olds and shows a marked male preponderance. It relates to repeated occupational trauma. Mycetomas caused by fungi are in general less inflammatory and less deeply invasive than bacterial lesions.
Pathogenesis and histologic features The most common fungal causes of mycetoma include:
• Madurella mycetomatis,
• Madurella grisea,
• Pseudallescheria boydii,
• Pyrenochaeta romeroi,
• Leptosphaeria senegalensis,
• Neotestudina rosatti. Bacterial causes include species of Nocardia, Actinomyces, and Streptomyces.5–11 Fungal causes account for a minority of cases of mycetoma.2 Of these, M. mycetomatis is the most important worldwide.8,12–14 An analysis of 73 cases from India, however, showed a decrease in the proportion of maduromycotic mycetoma versus actinomycotic mycetoma over a 4-year period.15 Infections due to Scedosporium apiospermum (the asexual counterpart of the teleomorph Pseudallescheria boydii), Cladophialophora bantiana, and Phaeoacremonium fuscum have been documented
953 Mycetoma
in iatrogenically immunosuppressed individuals.16–18 S. apiospermum eumycetoma may also occur in immunocompetent hosts.19 There is a report of Diaporthe phaseolorum (Phomopsis phaseoli) eumycetoma in a patient with human T-cell lymphotropic virus 1 (HTLV-1) infection.20
All the organisms produce granules, the configuration and color of which may be helpful in identifying the causative agent (Figs 18.347–18.350; Table 18.3).2 Although definitive speciation by means of culture is often challenging, newer PCR-based techniques hold promise.21 The black color of the granules seen in M. mycetomatis infection is due to the production of melanin, which may confer protection of the organism against the effects of antifungal agents.14,22,23 A polymorphism in the gene encoding for the chitin-degrading enzyme, chitotriosidase has been linked to an increased
risk for the development M. mycetomatis mycetoma.24 The granules are seen within areas of suppuration and are surrounded by palisaded histiocytes. They consist of an organized compact mass of hyphae, which may be associated with adherent neutrophils or a crystalline matrix.12,25,26 Multinucleate giant cells occur beyond this and there is a peripheral region of edematous granulation tissue. The use of special stains is of value in distinguishing actinomycetic from fungal (eumycetic) causes of mycetoma. The latter stain positively with PAS and silver stains but are negative with Gram stain (Fig. 18.351). A Splendore-Hoeppli phenomenon is sometimes evident (Fig. 18.352).
Response to therapy is variable, but the condition is more problematical when deep tissues are involved.
954 Infectious diseases of the skin
A
Maduromycotic (eumycetic) Actinomycetic
Black Madurella mycetomatis Madurella grisea Pyrenochaeta romeroi Phialophora jeanselmei Leptosphaeria senegalensis Leptosphaeria tompkinsii
Yellow or yellowish-white
Allescheria boydii Acremonium sp. Fusarium sp. Neotestudina rosatti Actinomadura madurae Streptomyces somaliensis
B
Red Actinomadura pelletieri
White or not visible
Nocardia brasiliensis Nocardia caviae Nocardia asteroides
Reproduced with permission from Magaña, M. and Magaña-Garcia, M. (1989) Dermatologic Clinics, 7, 203–217.
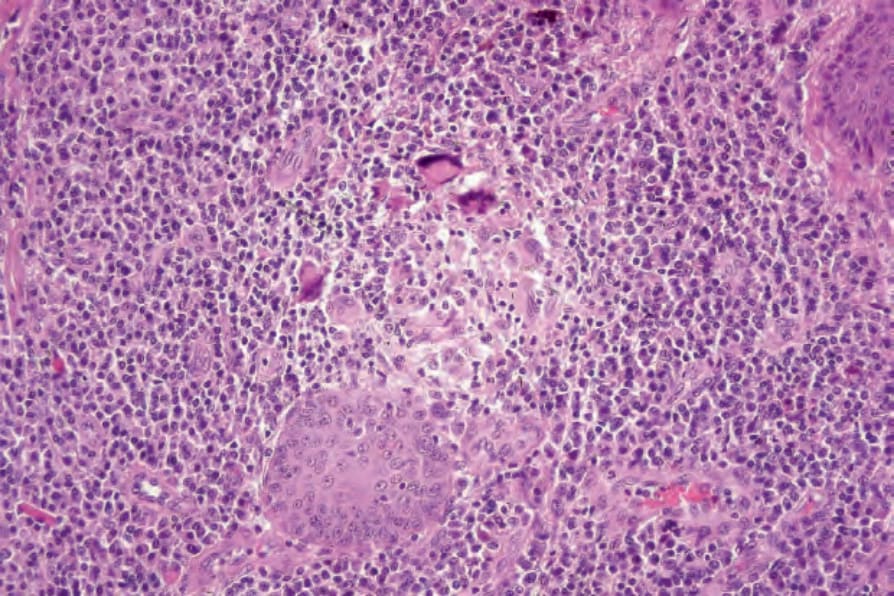
Fig. 18.343 Chromoblastomycosis: granulomata are commonly present.
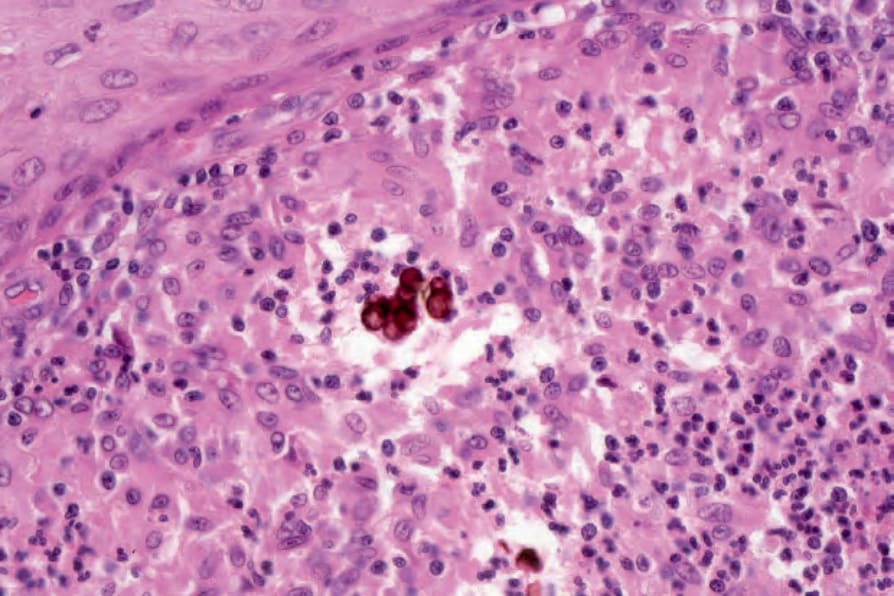
Fig. 18.344 Chromoblastomycosis: the brown-staining (sometimes septate) cells are pathognomonic.

Fig. 18.345 Mycetoma: the foot is grossly swollen and misshapen. Numerous draining sinuses are present.

Fig. 18.346 Mycetoma: multiple ulcerated verrucous nodules are present. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.
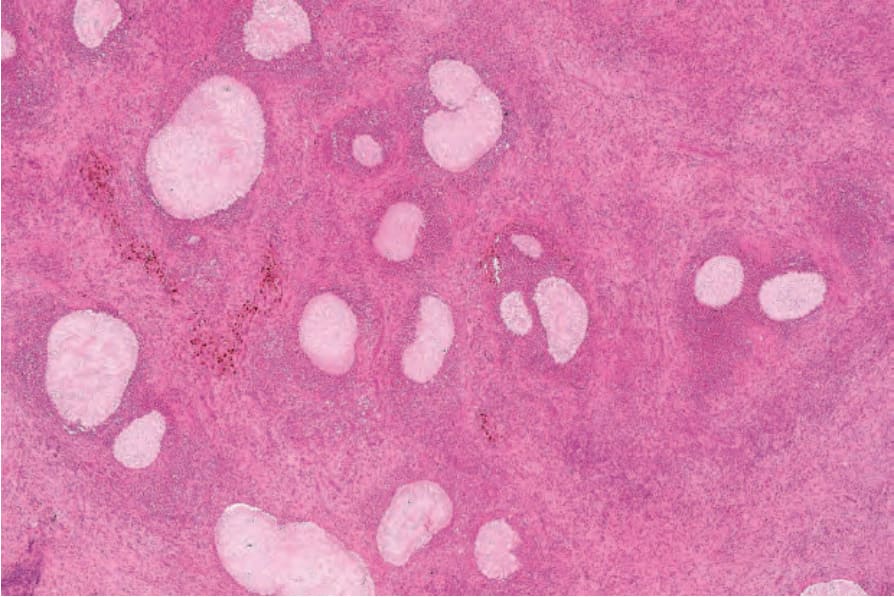
Fig. 18.347 Mycetoma: characteristic granules are present in neutrophil abscesses. There is a peripheral histiocytic/giant cell palisade.
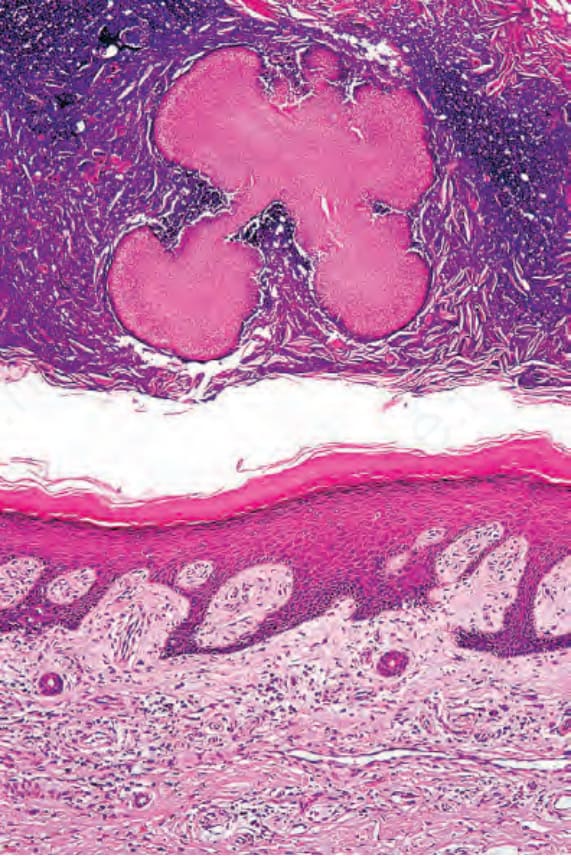
Fig. 18.348 Mycetoma: in this example, a colony is present in the overlying crust.
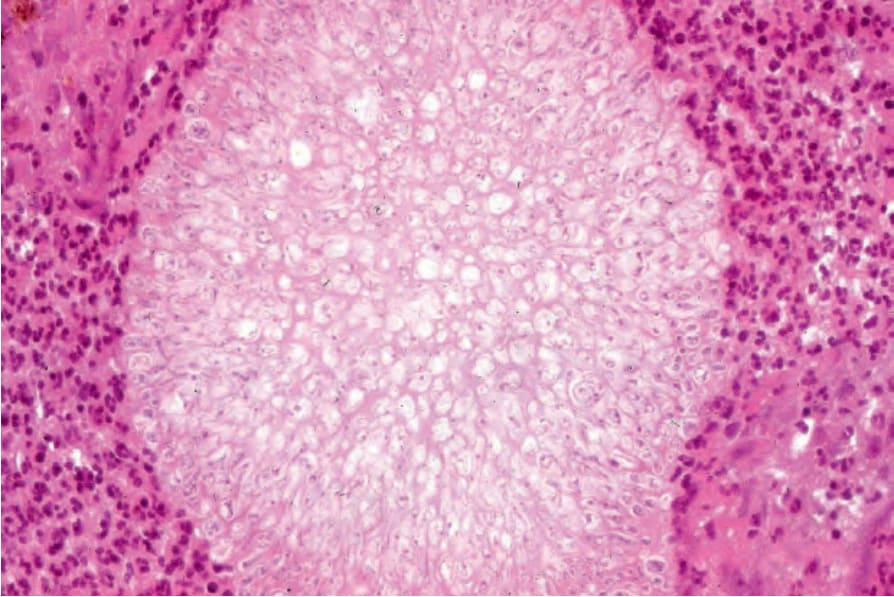
Fig. 18.349 Mycetoma: the internal structure of the granule is clearly visible in this high-power view.
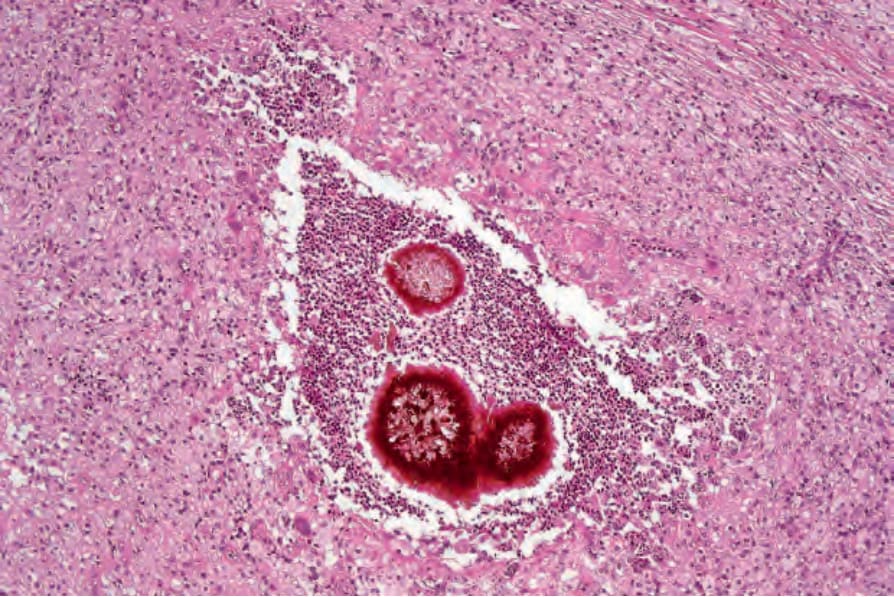
Fig. 18.350 Mycetoma: pigmented granules are characteristic of Madurella mycetomatis infection.
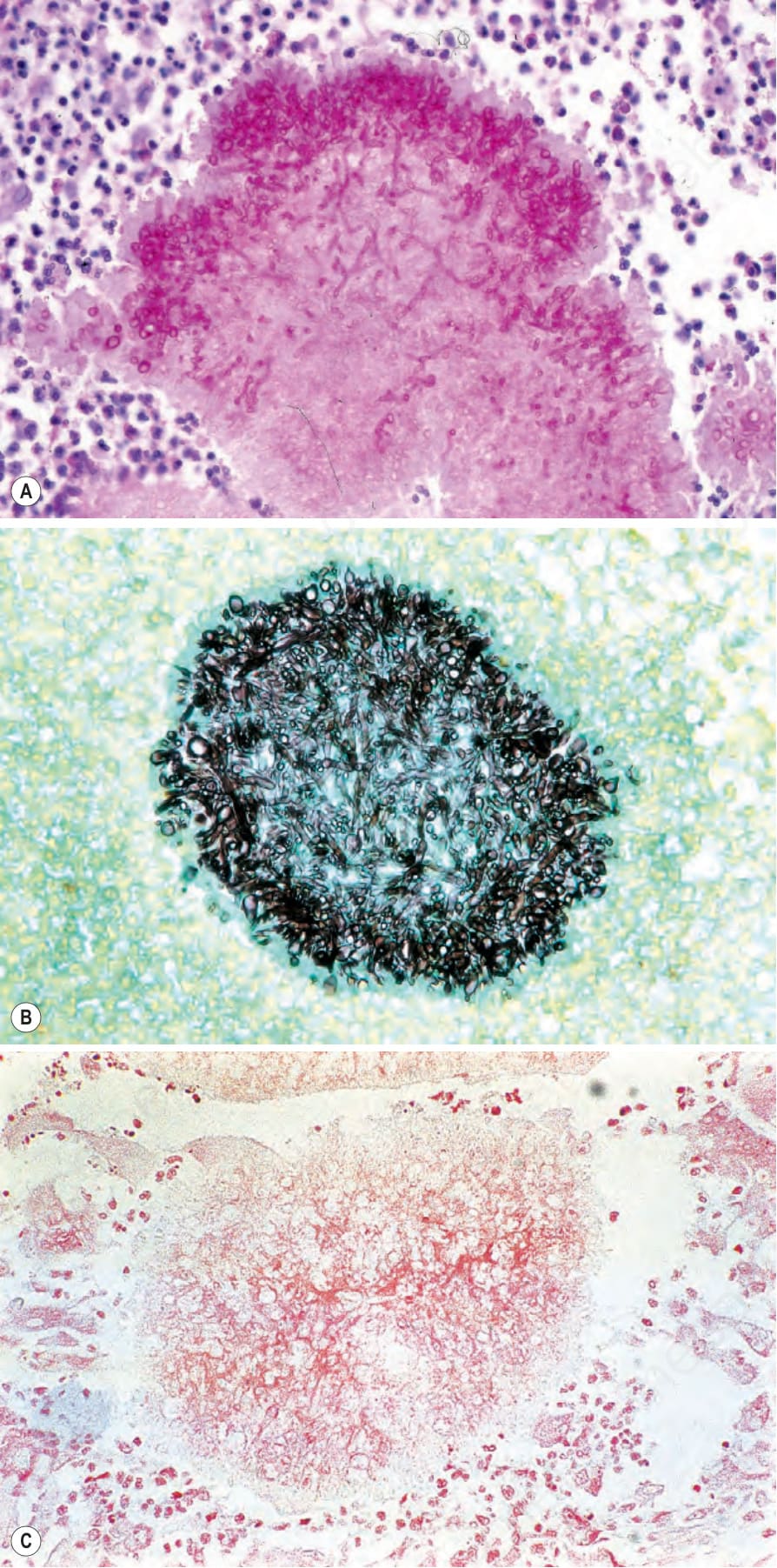
Fig. 18.351 (A–C) Mycetoma: the use of special stains readily confirms the fungal nature of this variant. (A) Periodic acid-Schiff; (B) methenamine silver; (C) Gram.
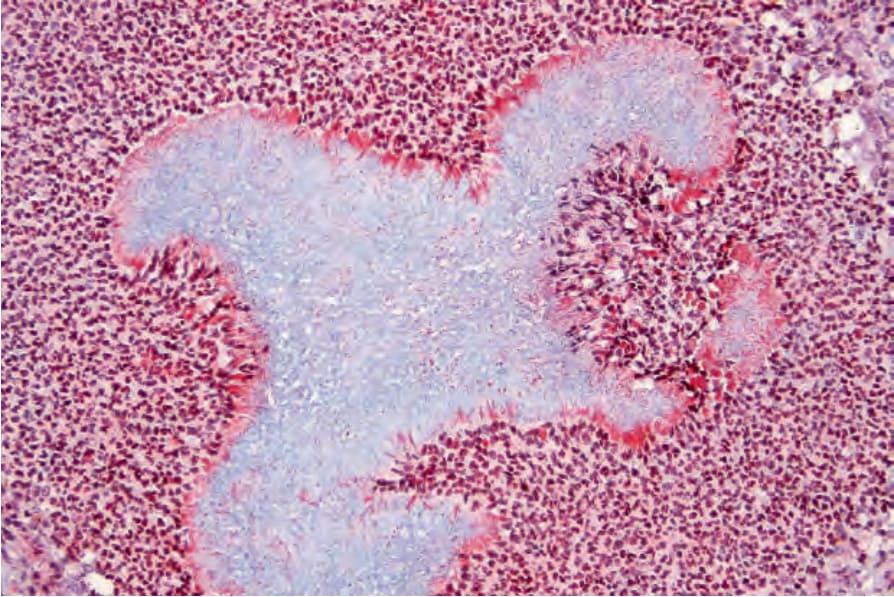
Fig. 18.352 Mycetoma: this fibrin stain highlights the Splendore-Hoeppli phenomenon.
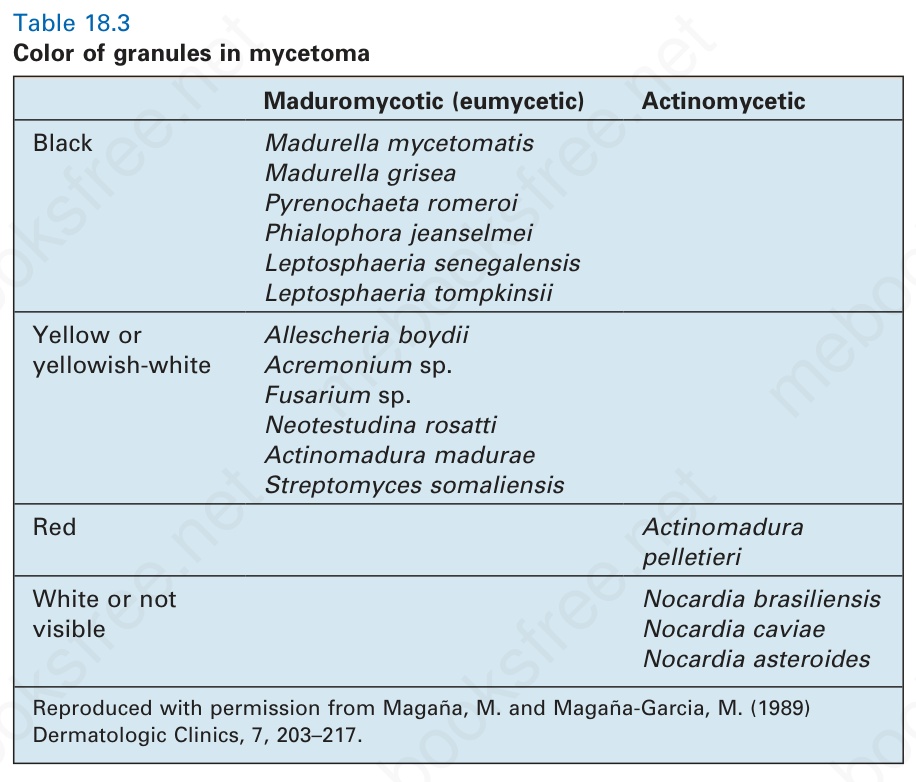
Table 18.3 Color of granules in mycetoma