Chromoblastomycosis
Chromoblastomycosis
Clinical features Chromoblastomycosis (chromomycosis) is a term applied to infection with some black (dematiaceous) fungi and is characterized by finding sclerotic pigmented bodies intermediate between a yeast and hyphal form in the tissues. Five main fungal species are associated with chromoblastomycosis1–5:
• Fonsecaea pedrosoi,
• Cladophialophora carrionii (formerly Cladosporium carrionii),
• Fonsecaea compacta,
• Phialophora verrucosa,
• Rhinocladiella aquaspersa.
951 Chromoblastomycosis
Other organisms, such as Exophiala spinifera, Aureobasidium pullulans, Chaetomium funicular, F. monophora, F. pugnacius, F. nubica, Cladosporium cladosporoides, C. bantiana, and Veronaea monophora, have rarely been implicated.6–15 Infections have occurred throughout the world, almost entirely in adult males (more than 90% in some series).16,17 The disease is nevertheless more prevalent in tropical countries, especially in parts of South America.2,3,5 The fungi are thought to be present in soil, wood, and vegetable debris. Thorns of the plant Mimosa pudica probably represent a natural source of chromoblastomycosis caused by F. pedrosoi.18 Other infections caused by dematiaceous fungi include mycetoma and pheohyphomycosis, and are discussed separately in this chapter.1,19 The pigment represents melanin.20 Chromomycosis is particularly seen in farmers and agricultural workers.16,21,22 Children and teenagers, however, may also be affected in areas where the disease is endemic.23 Although the majority of infections occur in otherwise healthy individuals, cases have been documented in the presence of underlying immunosuppression, including systemic corticosteroid therapy; there is a tendency toward infection with less conventional organisms in this clinical context.10,14,15,24
The infection occurs primarily in skin following trauma. It begins as scaly pink papules, most often on the lower leg or foot. These enlarge slowly to become nodules and then purplish irregular plaques and verrucous nodules (Fig. 18.340). Eventually, many of these become large papillomatous lesions, which are pruritic. The associated scratching may result in adjacent satellitosis. The condition progresses slowly for many years and may end as grossly deforming large tumor masses.25–27 Lymphangitic spread has been reported.28,29 A rare presentation with annular lesions has been described.30 Secondary bacterial infection often causes foul smelling discharge, ulceration, and lymphadenitis. Involvement of underlying tissues does not occur, although hematogenous spread to the CNS has been reported on rare occasions.11,31 Secondary (bacterial) regional lymphadenopathy may be evident.21 Squamous cell carcinoma is a rare complication of chronic disease.22,32–35 There have been rare reports of penile, vulval, and nasal chromoblastomycosis. Extracutaneous lesions involving the pleura, ileocecal region, laryngotracheal region, and tonsils have also been described.36 Contiguous involvement of underlying bone is a rare occurrence.37
proteins such as IgG, and components of the extracellular matrix, including laminin and fibronectin.42 One study has suggested that a suboptimal host immune response to the organisms is the result of an imbalance in regulatory (Treg) and Th17 T-cells.43
The sclerotic bodies (also referred to as Medlar bodies) are round or polyhedral, pigmented, thick-walled fungal cells 5–12 µm in diameter.19,44 Despite its name, blast formation does not occur.1 The sclerotic body is phenotypically midway between a yeast and a hypha and therefore has cross walls in two planes.1 The tissue reaction resembles that seen in blastomycosis.19 There is marked epidermal acanthosis, with neutrophil microabscesses (Figs 18.341 and 18.342). The hyperplasia often becomes pseudoepitheliomatous.31,44 The dermis shows abscess formation with necrosis and a surrounding granulomatous and mixed inflammatory infiltrate consisting of neutrophils, eosinophils, lymphocytes, and plasma cells. The admixture of neutrophil microabscesses and granulomatous inflammation is described as a mixed (mycotic) granuloma (it is also a feature of blastomycosis, sporotrichosis, pheohyphomycosis, coccidioidomycosis, and paracoccidioidomycosis).31 The sclerotic bodies are seen both within giant cells and extracellularly (Figs 18.343 and 18.344). Transepidermal elimination of fungal cells has been described.45 Dematiaceous hyphae may also be seen in the dermis.19 Dermal fibrosis is often marked and in many cases the
Pathogenesis and histologic features The most common fungus causing chromoblastomycosis is F. pedrosoi.19,21,38 This organism has been isolated from 70% to 90% or more of cases in some series.22,39,40 A multinational study showed that F. pedrosoi can be classified into seven mitochondrial DNA types; these appear to correspond to geographic origin.41 Experimental evidence indicates that the production of proteolytic enzymes (peptidases) by F. pedrosoi results in cleavage of serum
952 Infectious diseases of the skin
subcutaneous fat is also affected. An unusual case characterized by an exuberant intradermal fascicular spindled cell proliferation has been reported.46 Classification of the causative organism depends on culture, and more recently via panfungal PCR with subsequent sequence analysis.47
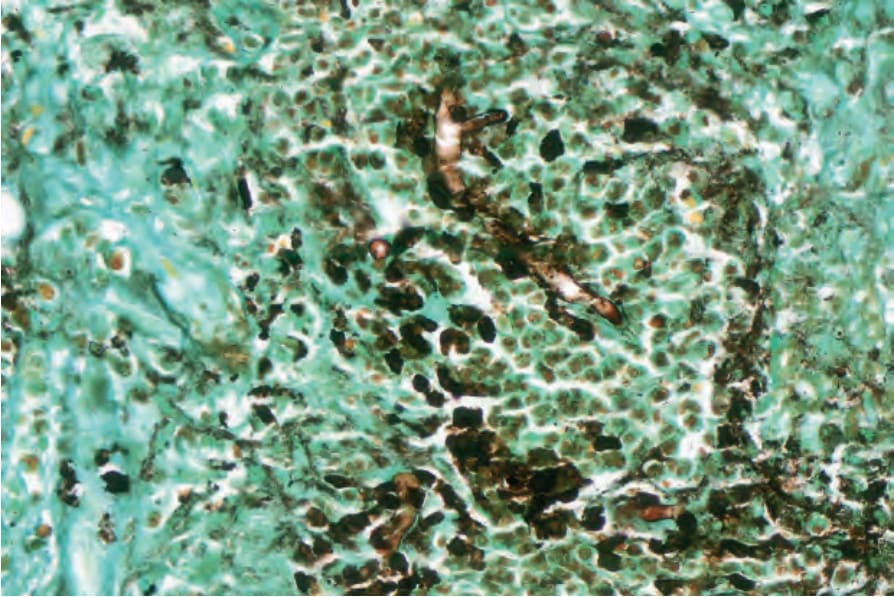
Fig. 18.339 Basidiobolomycosis: the hyphae are irregular and often appear twisted (methenamine silver).

Fig. 18.340 Chromoblastomycosis: there are multiple nodules and disfiguring plaques. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.
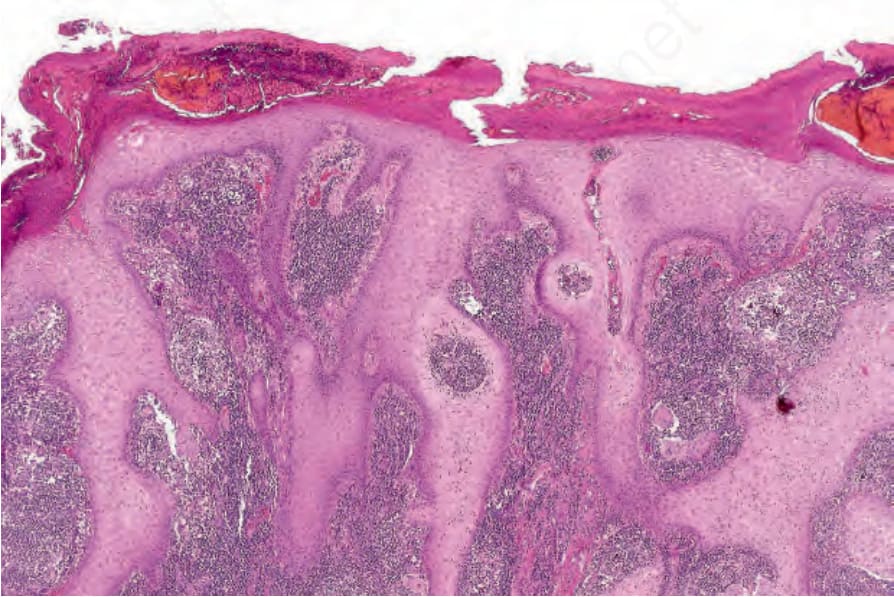
Fig. 18.341 Chromoblastomycosis: the epidermis is hyperkeratotic, crusted, and shows very marked acanthosis.
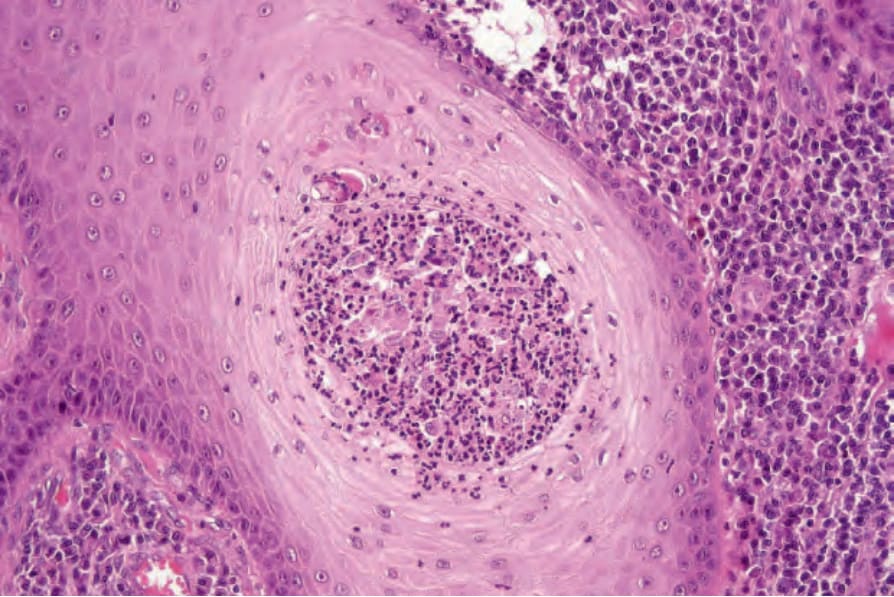
Fig. 18.342 Chromoblastomycosis: abscesses within both the epidermis and dermis are characteristic.
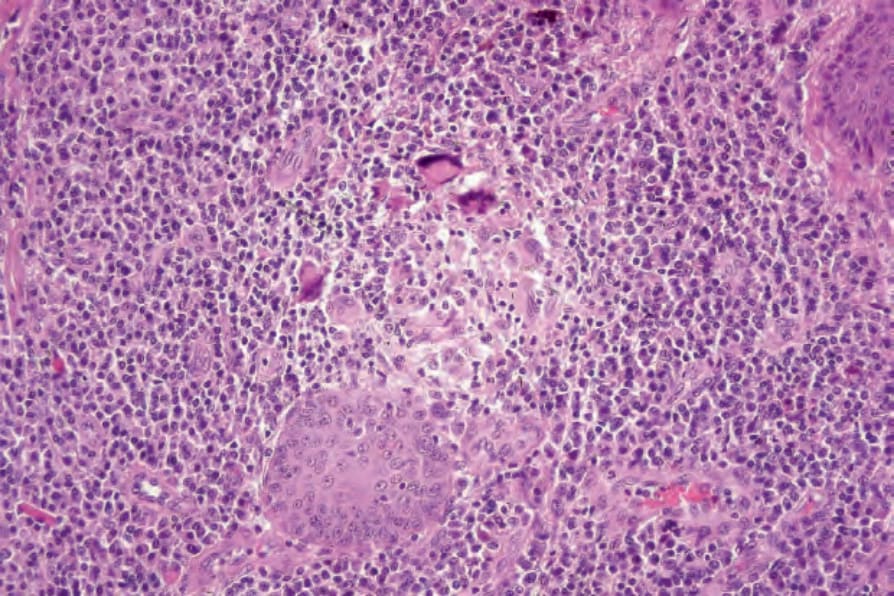
Fig. 18.343 Chromoblastomycosis: granulomata are commonly present.

Fig. 18.345 Mycetoma: the foot is grossly swollen and misshapen. Numerous draining sinuses are present.