Entomophthoramycosis
Entomophthoramycosis
Clinical features Entomophthoramycosis (entamophthoromycosis; subcutaneous zygomycosis) encompasses rare infections caused by:
• Basidiobolus ranarum or B. haptosporus, and referred to as basidiobolomycosis; or
• Conidiobolus coronatus, C. incongruus or C. lamprauges, and referred to as conidiobolomycosis. These organisms are members of the order Entomophthorales, and are also responsible for cutaneous and nasopharyngeal infections in animals such as horses.1–9 Entomophthoramycosis occurs predominantly in tropical and subtropical regions of Africa, Asia, and South America.1 Unlike mucormycosis, basidiobolomycosis and conidiobolomycosis do not appear to be opportunistic pathogens in the majority of cases; infection is usually acquired by
950 Infectious diseases of the skin
inoculation, either through minor trauma or occasionally via an insect bite.1 There have nevertheless been rare reports of entomophthoramycosis following iatrogenic immunosuppression.5,12,10,11 Both B. ranarum and C. coronatus are found in soil and decaying vegetable material.1,7 B. ranarum also occurs in the gut of fish, amphibians, reptiles, and bats.1,8
Basidiobolomycosis is seen most frequently in children or adolescents, who present with confluent cutaneous and subcutaneous plaques. The lesions are fluctuant, generally nontender and well demarcated, and occur predominantly on the limbs, trunk, or buttocks (Fig. 18.336).1,7,8 Tumorlike masses may evolve.1 There have been rare reports of nasal or paranasal sinus lesions.13,14 There is a male predilection.8 Involvement of the lymph nodes, with lymphedema and elephantiasis, has also been reported.15,16 There is a single case report of penile basidiobolomycosis.17 Although rare, primary or secondary visceral involvement may occur.1,10,18,19 Numerous cases of gastrointestinal basidiobolomycois have been reported.20
Conidiobolomycosis, by contrast, is an infection that tends to occur in adults, who manifest with mucocutaneous lesions of the nose with subsequent spread to the paranasal sinuses and rhinofacial subcutaneous tissues (rhinoentomophthoromycosis).1,3 Although the vast majority of documented infections have occurred in healthy, immunocompetent hosts, 2.5% of reported infections have arisen in the setting of underlying hematolymphoid neoplasia.12 There is erythema and thickening of the nasal skin. This may progress to massive deforming tumefaction of the nose, cheeks and/or lips, and facial elephantiasis.1,12,21–24 The infection can also spread to involve the eyelid and orbit.1,25 Intracranial extension has been documented.26 Fatal visceral dissemination is a rare complication.5
18.338 and 18.339).1,12,19 Phagocytosed hyphal fragments are sometimes visible within the cytoplasm of giant cells.7 One reported case of conidiobolomycosis was accompanied by chronic localized fibrozing leukocytoclastic vasculitis and a resultant histologic picture reminiscent of granuloma faciale.12 Diagnosis is facilitated by recognition of the distinctive histologic findings and culture of the causative organism; molecular (PCR) mycology techniques, however, have recently assumed a more prominent role.3
Histologic features The variably septate fungal hyphae in entomophthoramycosis are not as broad as those encountered in mucormycosis, and have an average diameter of 8–10 µm. An additional point of distinction is the fact that angioinvasion does not tend to occur in entomophthoramycosis.1 There is extensive granulomatous inflammation with neutrophilic microabscesses and large numbers of eosinophilic leukocytes (Fig. 18.337).12 The hyphae are clearly discernible in H&E-stained sections but can be highlighted with methenamine silver, and are frequently associated with the Splendore-Hoeppli phenomenon (Figs
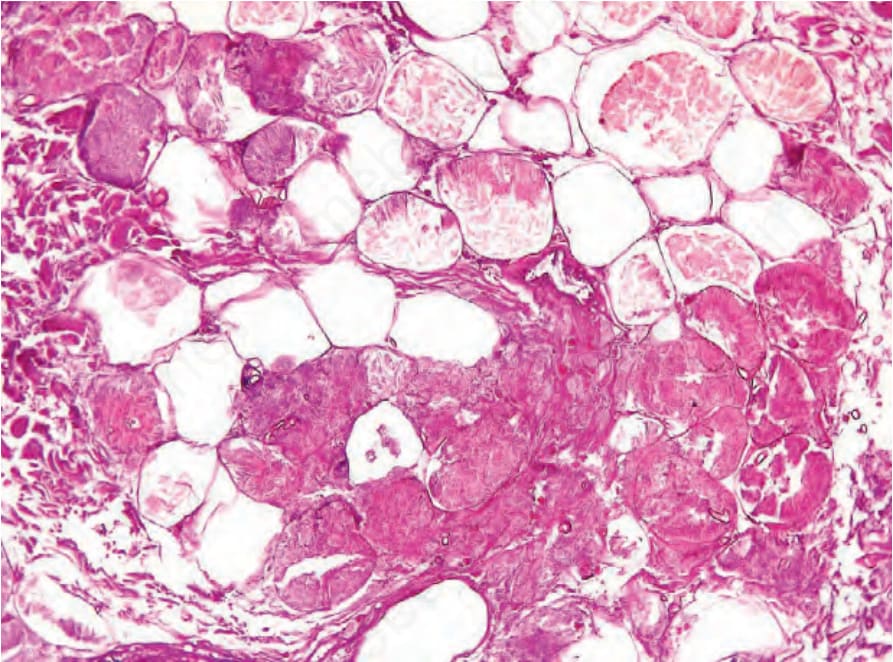
Fig. 18.335 Mucormycosis: subcutaneous involvement in this example is associated with extensive fat necrosis and a picture strikingly reminiscent of gouty panniculitis and pancreatic panniculitis. By courtesy of V. Yazbek, MD, Ampath National Laboratories, Bloemfontein, South Africa.

Fig. 18.336 Basidiobolomycosis: there is a large abscess in the left buttock. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.
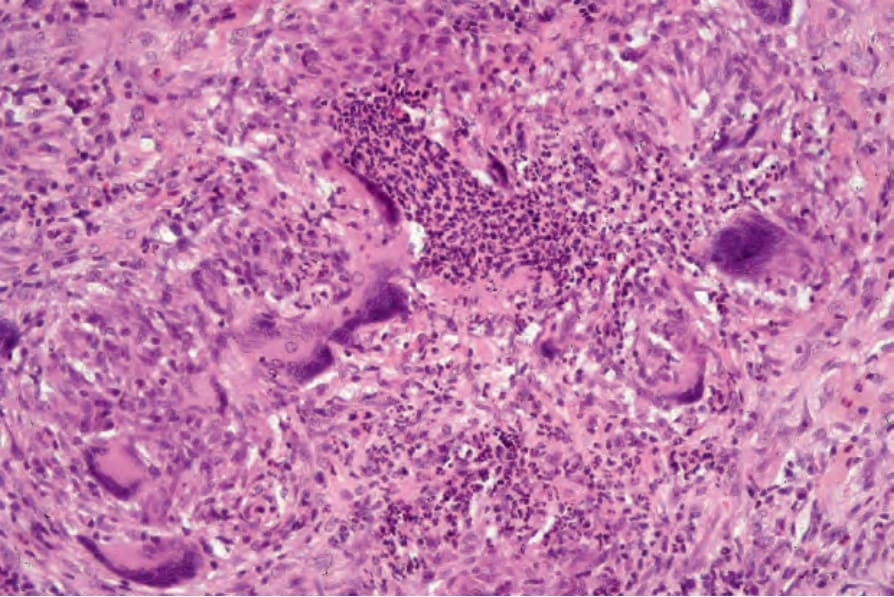
Fig. 18.337 Basidiobolomycosis: high-power view showing a heavy mixed granulomatous and suppurative dermal infiltrate with admixed eosinophils.
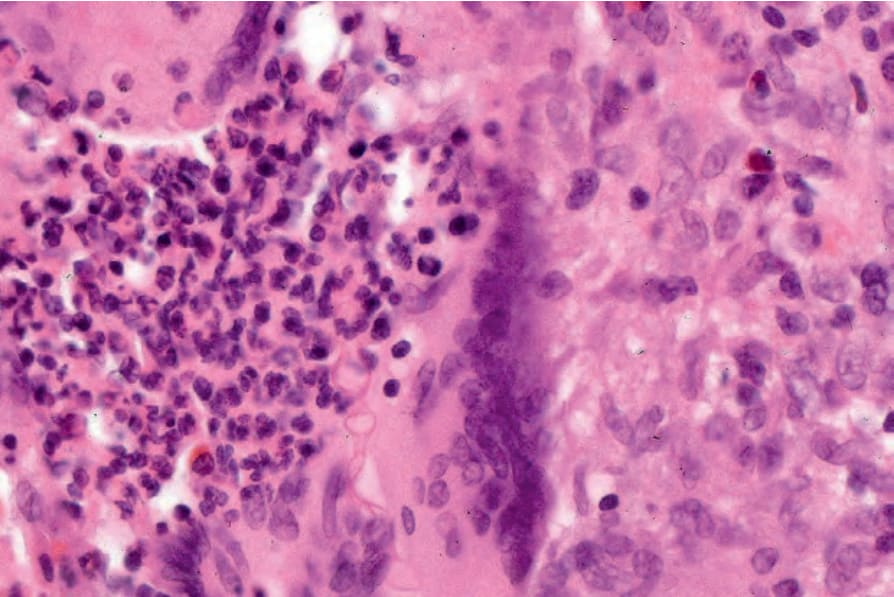
Fig. 18.338 Basidiobolmycosis: the fungi are often clearly visible in hematoxylin and eosin stained sections.