Cryptococcosis
Cryptococcosis
Clinical features Cryptococcus neoformans var. neoformans causes systemic infections sporadically throughout the world because it is abundant in soil, fruits, and
946 Infectious diseases of the skin
pigeon droppings.1,2 It causes disease in adults and, rarely, in children. The infection often complicates immunosuppression including that due to corticosteroid therapy, neoplastic disease (particularly the terminal phases of Hodgkin lymphoma), solid organ transplant recipients, and HIV/AIDS.1–8 Cryptococcosis (torulosis) is the most frequent and potentially lethal mycosis in patients with HIV/AIDS.9
Primary cryptococcal cellulitis has been reported in an immunocompetent host.37 Another reported immunocompetent patient developed nodules and ulcers on the forearm following injury sustained through handling of barbed wire and eucalyptus logs.39 There is a report of C. gattii-associated NF in a patient with diabetes mellitus.40 Disseminated disease has also been reported in immunocompetent individuals, who may present with papules, pustules, plaques, ulcers, subcutaneous involvement, cellulitis, or acneiform lesions.41 C. laurentii infection is rare and is usually acquired nosocomially. Patients are often neutropenic and develop fungemia in the presence of an indwelling intravenous catheter.42 Primary infection, however, has been documented in a renal transplant recipient, and occasionally in immunocompetent hosts.31,43 Fewer than 20 cases of systemic C. albidus infection have been reported, including a renal transplant recipient; primary cutaneous infections due to this organism are exceptionally rare.44,45 There has been one report of C. diffluens infection in an immunocompetent patient, who developed sporotrichoid lesions.46
The portal of entry is usually the lungs, and systemic spread to the brain is common. Indeed, CNS involvement (meningitis and meningoencephalitis) is the major source of morbidity and mortality. Other sites commonly affected in disseminated disease include the skin, bone, and prostate.9 Untreated cryptococcosis, particularly if HIV/AIDS related, has a very high mortality.
Secondary cutaneous lesions occur in approximately 10% (6–15%) of cases.8,10–12 Skin lesions may also precede evidence of cerebral pathology.2 Cutaneous manifestations comprise a wide range of lesions including papules, pustules, vesicles, nodules, plaques, cellulitis, ulcers, papable purpura (pseudo-Kaposi), and subcutaneous lesions, which may resemble erythema nodosum (Fig. 18.323).5,11–17 Herpetiform, keloidal, MC-like lesions, pyoderma gangrenosum-like lesions, and NF have also been recorded.8,12,14,18–23 The head and neck are the most commonly affected sites (Fig. 18.324).24 Ulcerated lesions have a punched-out appearance with gelatinous-looking margins resembling basal cell carcinomas.
Pathogenesis and histologic features C. neoformans is a spherical yeast, which measures from 4 to 20 µm in diameter. It is characterized by a mucoid capsule and by reproducing by (narrow-based) budding.2,47,48 There are four serotypes (A–D).1,2 In patients with HIV/AIDS, serotypes A and D are almost always implicated.9
Lesions developing as a result of primary inoculation of the skin are very rare, but appear to have a good prognosis since the overwhelming majority of these infections have occurred in immunocompetent individuals.25–33 Inoculation as a consequence of needlestick injury has been reported among healthcare workers.26 Primary cutaneous cryptococcosis has been reported following iatrogenic immunosuppression.7,34,35 Features said to be indicative of secondary cutaneous involvement rather than primary disease are deep dermal or subcutaneous inflammation and multifocal skin lesions, especially when present on covered parts of the body.36
Humans may also be infected by species of Cryptococcus other than C. neoformans var. neoformans. C. neoformans var. gattii is endemic in Australia, where it is associated with two species of eucalyptus tree.37,38 Disseminated infection due to C. gattii may occur in immunocompromised patients.
Cell-mediated immunity is of particular importance in the host response and corresponding likelihood of systemic lesions.2,38 The first line of defense against C. neoformans is offered by alveolar macrophages following inhalation of the organisms.38 The release of proinflammatory monokines by these macrophages results in the local recruitment of monocytes and polymorphonuclear leukocytes, offering a second line of defense. The production of lymphokines and specific antibodies constitutes the third tier of defense. IL-12 and IL-18 play a critical role through their action on lymphocyte responses.38 Patients with low CD4+ T-lymphocyte counts are particularly susceptible to infection.49
The mucoid capsule is the characteristic feature in the tissues. It is, however, unencapsulated in nature.2 It may also be unencapsulated in patients with HIV/AIDS.9 The development of a polysaccharide capsule
947 Mucormycosis
appears to correlate with its pathogenicity.48,50 There may be chains of budding cells in some lesions. Often there is a gelatinous reaction with little inflammation, but in other lesions there is a granulomatous response with necrosis and in some patients there is a suppurative reaction (Figs 18.325–18.330).51 In the gelatinous reaction, organisms are very numerous, but in the others the cryptococcus may be more difficult to see and mucicarmine, PAS, Alcian blue, and methenamine silver stains can be useful (Figs 18.331–18.333). Mucicarmine positivity in particular discriminates between cryptococcus and other tissue fungal infections with similar morphology, which are characteristically negative (e.g., histoplasmosis and blastomycosis).2,47,52 A unique palisading granulomatous response to chronic cryptococcosis has been described.53 Necrotizing vasculitis has also been reported.54
Diagnosis is usually very simple and is based on morphological features.55 In cases of doubt, cryptococcal antigen may be identified in serum or cerebrospinal fluid using the latex agglutination test.9 The diagnosis may also be confirmed by means of in situ hybridization performed on skin biopsy material.47,56 Use of the Tzanck smear as a rapid diagnostic tool has been advocated by some authors.57
In patients with underlying HIV/AIDS, it is important to examine the tissue sections carefully for additional pathology. C. neoformans infection has, for example, been reported in association with Kaposi sarcoma, MAI infection, and MC.58–61
Differential diagnosis
Infection with capsule-deficient forms of the organism may result in potential confusion with Candida spp. or H. capsulatum.47,48 On rare occasions, neutrophilic dermatoses such as Sweet syndrome may closely mimic Cryptococcus infection due to the presence of acellular bodies with surrounding capsule-like spaces amid the dermal inflammatory infiltrate.62,63
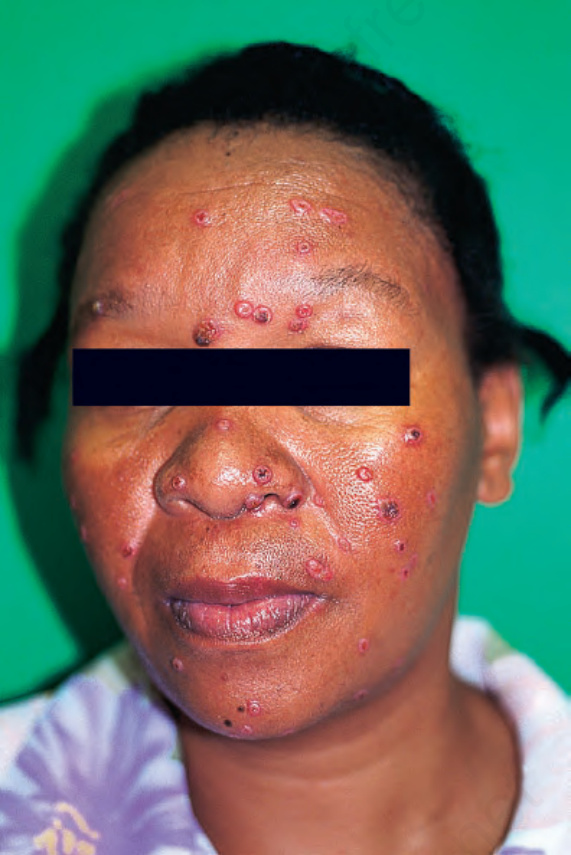
Fig. 18.323 Cryptococcosis: multiple erythematous nodules are present. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.

Fig. 18.324 Cryptococcosis: this patient has innumerable facial papules. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.
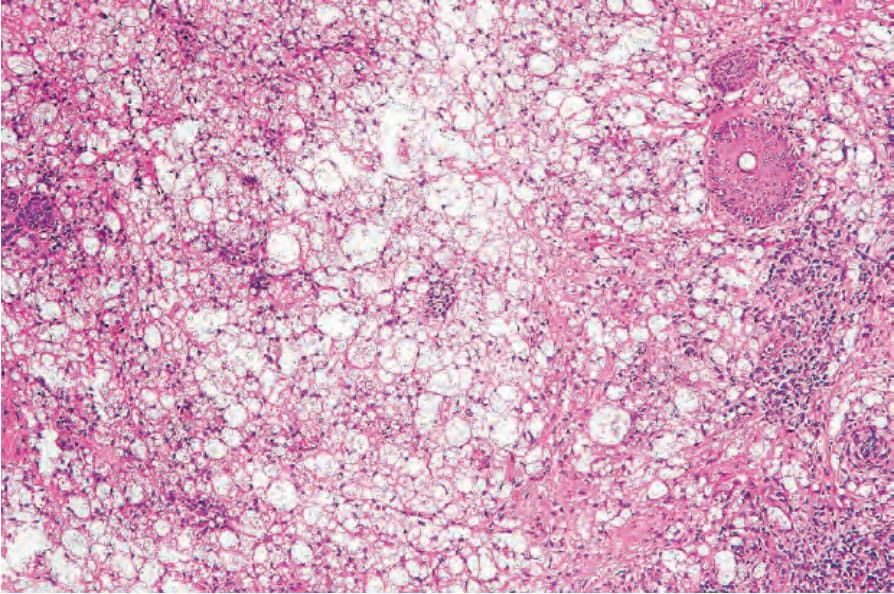
Fig. 18.325 Cryptococcosis: there is an intense mucoid dermal infiltrate.
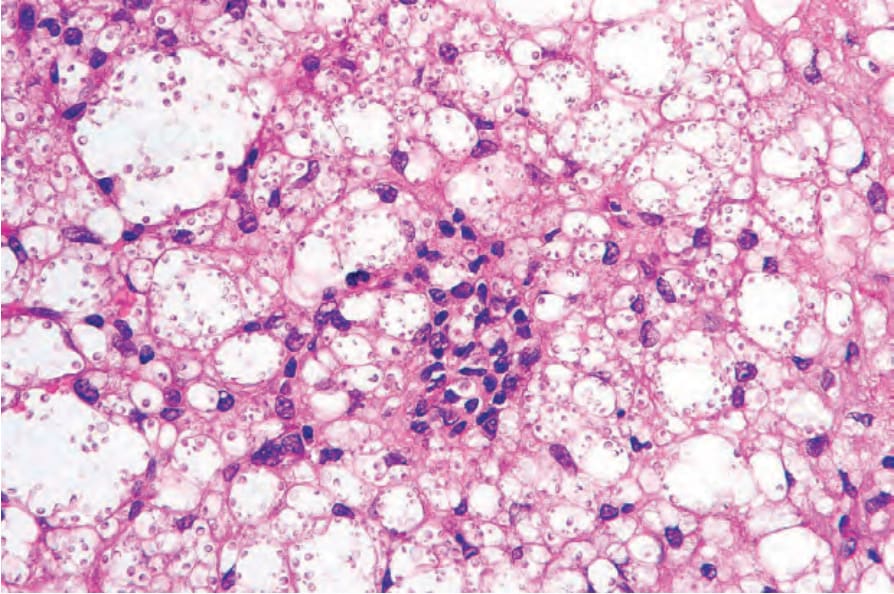
Fig. 18.326 Cryptococcosis: the yeast forms are widely separated by their thick capsules.
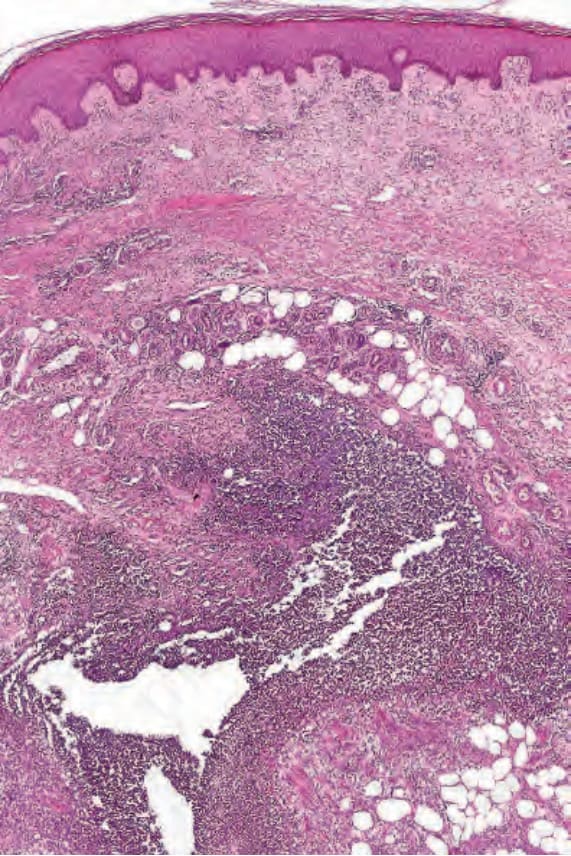
Fig. 18.327 Cryptococcosis: this suppurative variant developed in a patient with lymphoma.
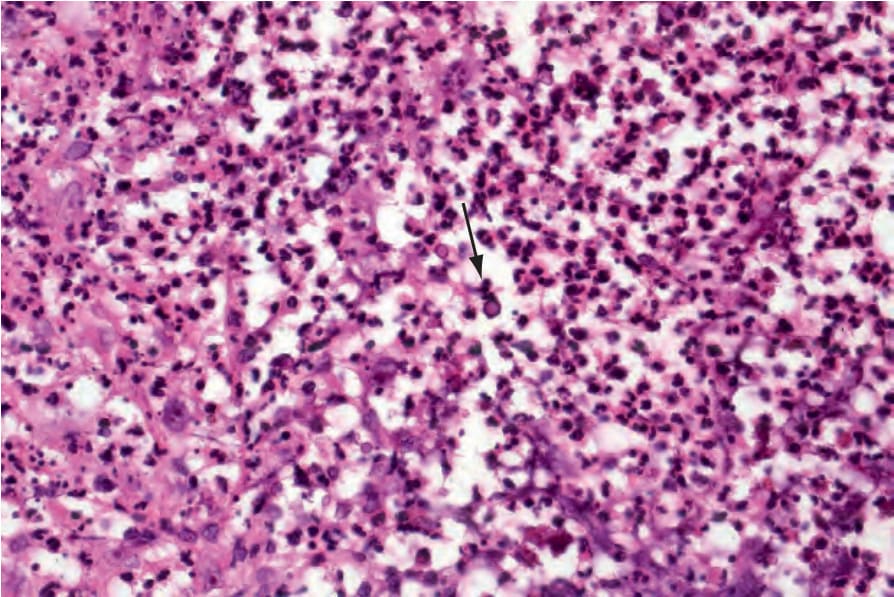
Fig. 18.328 Cryptococcosis: high-power view showing a dense neutrophil infiltrate. A yeast is evident in the center of the field.
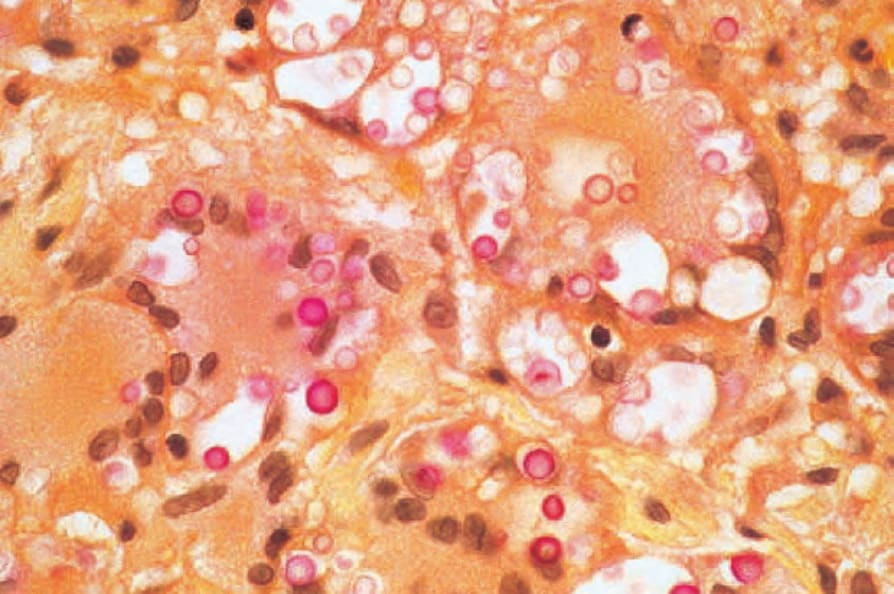
Fig. 18.331 Cryptococcosis: the capsule is clearly demonstrated with the mucicarmine stain.