Coccidioidomycosis
Coccidioidomycosis
Clinical features Coccidioidomycosis is a virulent fungal infection caused by two etiological species: Coccidioides immitis, which is found in its mycelial form in the soil of desert regions of the southwestern United States (especially California and the Lower Sonoran Life Zone), and C. posadasii, which is endemic in parts of northwest Mexico, arid and semi-arid regions of Central and South America, as well as Arizona and Utah.1–7 Primary infection occurs by inhalation of airborne arthroconidia in dust and, in view of increased tourism in endemic areas, is becoming more common.1,8 A significant increase in the
944 Infectious diseases of the skin
incidence of this infection has been observed in California and elsewhere since the early 1990s.1,9,10 In endemic regions, primary coccidiodal pneumonia may account for as many as 29% of all cases of community-acquired pneumonia.4 The diagnosis may be overlooked in the absence of a detailed travel history in patients presenting with symptomatic disease after returning to nonendemic areas.11 In those in whom symptoms (usually influenza-like) do develop, coccidioidomycosis is usually a self-limiting disease.12,13 Most episodes, however, are asymptomatic.9,13,14 It may also develop in the immunosuppressed, including patients with HIV/AIDS.9,15,16 Sixty percent of patients with pulmonary infection remain asymptomatic.8 Symptomatic lung involvement is encountered in the remaining 40% and may progress to cavitating, chronic progressive pneumonia, and miliary pulmonary disease.8,14 Pleural effusion, empyema, and acute respiratory distress syndrome may also occur.8 Chronic infection develops in 3% to 5% of patients.4
complication of systemic disease. Hemophagocytic lymphohistiocytosis has also been reported.25
The rare primary lesions in the skin occur following inoculation, usually in farmers, laboratory workers, nurses, and morticians.14,26 These lesions are chancriform and there is regional lymphadenopathy. Sometimes, sporotrichoid features are evident. Toxic erythema (exanthem), erythema nodosum, and erythema multiforme may occur as hypersensitivity reactions during systemic infection.2,14 The combination of erythema nodosum or erythema multiforme with arthritis and arthralgia is known as ‘valley fever’.12 Systemic eosinophilia may be evident. Additional reactive cutaneous manifestations include interstitial granulomatous dermatitis and Sweet syndrome.2,6 A case with associated subcorneal pustular dermatosis has also been reported.27
Cutaneous lesions are uncommon and develop almost invariably as a result of the rare dissemination from pulmonary lesions; this occurs in approximately 5% of patients.16–18 Dissemination occurs more often in blacks, Filipinos, Hispanics, and native Americans and shows a slight male preponderance.12,19 There is also an increased risk in the immunosuppressed, including those with diabetes mellitus or who are receiving corticosteroids.3 The lesions include papulonodules, papulopustules, granulomatous plaques, and subcutaneous masses (Figs 18.317 and 18.318).18,20,21 Sinus tracts complicating osteomyelitis or infection of adjacent joints or lymph nodes may also be seen.12,21 Although generally multiple, solitary nodular presentation has been rarely described.22 The central face, in particular the nasolabial fold, is most often affected.14,23 Involvement of the face may be indicative of a propensity to develop meningitis.19
Histologic features C. immitis and C. posadasii are dimorphic fungi, which in tissues appear as doubly refractile spherules 10–100 µm in diameter containing multiple endospores (2–5 µm) that increase in size as the lesions mature.3,28 The incubation period ranges from 1 to 4 weeks.2,14 Diagnosis may be aided by the coccidioidin skin test, enzyme immunoassay (complement fixation test), or PCR techniques.1,12,29–31 The histology resembles North American blastomycosis in that there is a combination of suppuration with pseudoepitheliomatous hyperplasia and an associated dermal perivascular infiltrate of neutrophils, eosinophils, plasma cells, histiocytes, and giant cells (Figs 18.319–18.321).1,18,28 Eosinophil abscesses may be present and flame figures have been described.11 Interstitial granulomatous dermatitis has also been reported.2,32
Disseminated lesions may also affect bone, joints, lymph nodes, pericardium, peritoneum, skeletal muscle, retropharyngeal space, and CNS.3,13,14 In the immunosuppressed this may be as a consequence of reactivation of previously quiescent foci.14 These secondary lesions are sometimes seen in areas of minor trauma, often, for example, on the face. They appear as verrucous plaques and nodules with crusting and ulceration. Sinus tracts may extend from the primary lung lesion through the chest wall.21 Involvement of the nasal tip may mimic lupus pernio.24 Hypercalcemia is a rare
The spherules (sporangia) are seen mixed with this inflammatory infiltrate and occasionally are present in giant cells. They are demonstrated best by methenamine silver techniques. The endospores are PAS positive, but the spherules are negative. The fungi show autofluorescence under ultraviolet light and may be stained with Congo red.33 They are typically very difficult to find and may often only be demonstrated after examining numerous sections. The spherules increase in size with the formation of numerous endospores. Following rupture into the tissues, each endospore has the
945 Cryptococcosis
A
B
capacity to develop into a spherule, therefore repeating the growth cycle in the host.17 In situ hybridization or PCR may facilitate prompt confirmation of the diagnosis on paraffin-embedded skin biopsy material, and aids in the distinction from other deep fungal infections.34,35
Differential diagnosis Diagnosis depends on the demonstration of spherules with endospores. Fragments of spore or immature forms cannot be distinguished from blastomycosis or paracoccidioidomycosis. Fungal culture or in situ hybridization studies are useful in such cases. When spherules and endospores are present rhinosporidiosis should also be considered, although the clinical and histologic features are usually different. The spherules and endospores of rhinosporidiosis are much larger than those of coccidioidomycosis.28 Distinction from tuberculosis verrucosa cutis and halogenoderma may sometimes be necessary.20 Aggregates of altered red blood cells in myospherulosis may mimic Coccidioides spp. (Fig. 18.322).36

Fig. 18.317 Coccidioidomycosis: ulcerated nodules are present on the knee and ankle. By courtesy of R. Arenas, MD, and J.C. Salas, MD, Monterrey, Mexico.

Fig. 18.318 Coccidioidomycosis: there is a crusted plaque on the arm. By courtesy of R. Arenas, MD, and J.C. Salas, MD, Monterrey, Mexico.
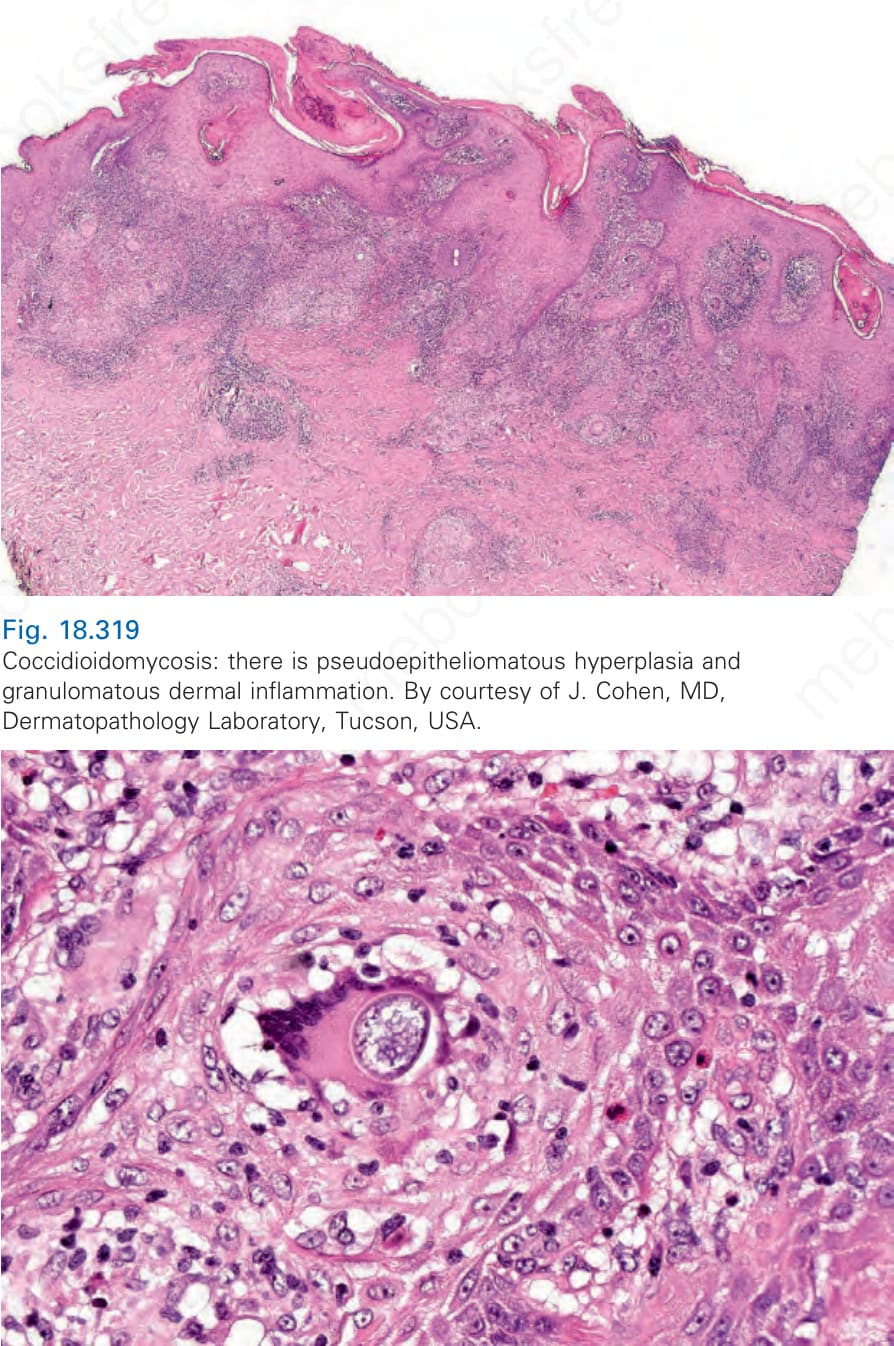
Fig. 18.319 Coccidioidomycosis: there is pseudoepitheliomatous hyperplasia and granulomatous dermal inflammation. By courtesy of J. Cohen, MD, Dermatopathology Laboratory, Tucson, USA.
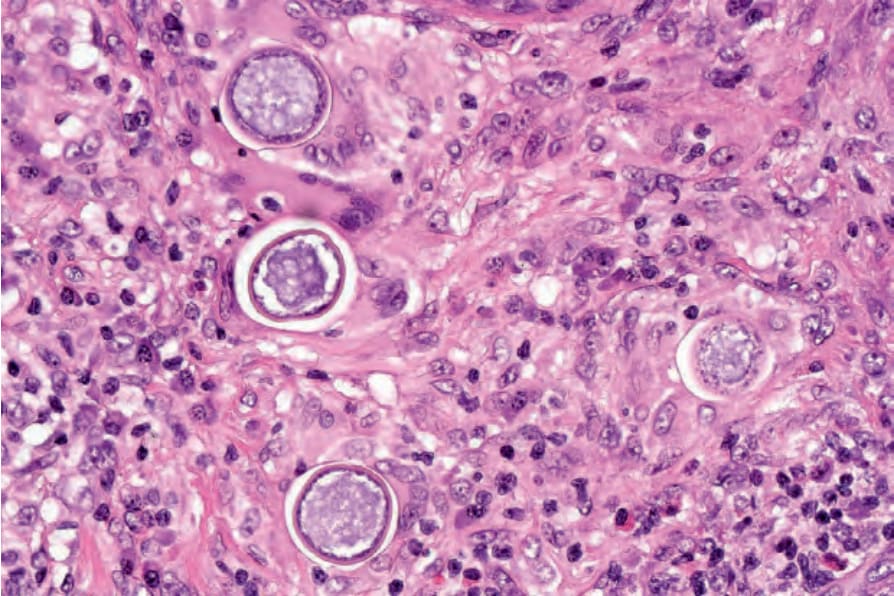
Fig. 18.320 Coccidioidomycosis: high-power view of a spherule within a multinucleate giant cell. By courtesy of J. Cohen, MD, Dermatopathology Laboratory, Tucson, USA.
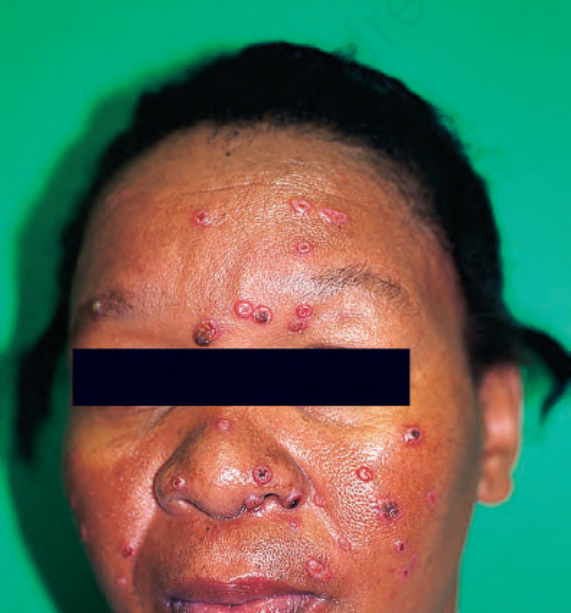
Fig. 18.321 Coccidioidomycosis: multiple spherules are present with surrounding chronic inflammation. By courtesy of J. Cohen, MD, Dermatopathology Laboratory, Tucson, USA.
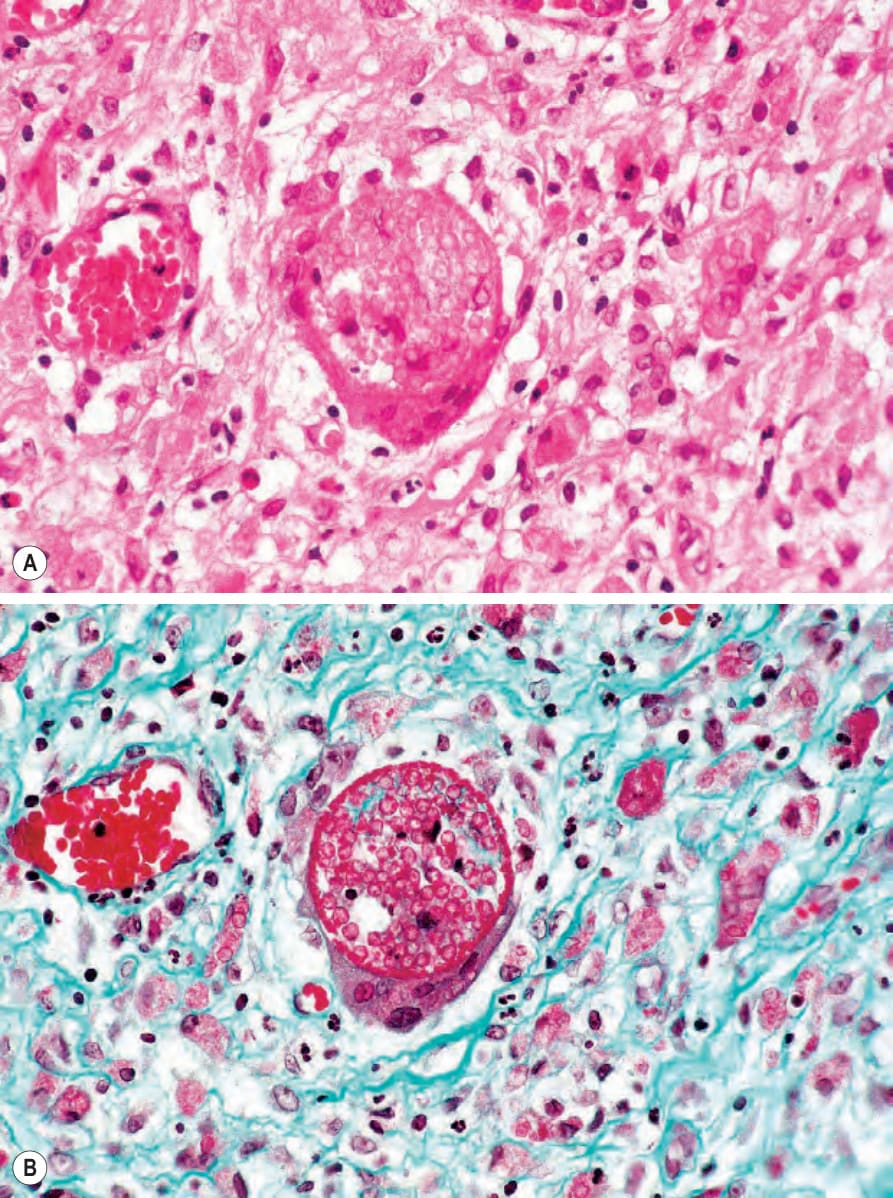
Fig. 18.322 (A, B) Myospherulosis: cutaneous lesions are exceptionally rare. This ‘cystic’ structure contains altered erythrocytes. The condition was originally recognized following the use of antibiotics – in this example, tetracycline ointment for an ear infection. (B) Masson trichrome. By courtesy of the late M.S.R. Hutt, MD, St Thomas’ Hospital, London, UK.