Paracoccidioidomycosis
Paracoccidioidomycosis
Clinical features Paracoccidioidomycosis (South American blastomycosis) is caused by Paracoccidioides brasiliensis and occurs in Central and South America, particularly Brazil. It is the most prevalent systemic mycosis in Latin America. It affects adult males much more commonly than females, usually in rural areas and more so among farmers.1–6 Rare cases have nevertheless been reported outside of this geographic location (e.g., due to increased immigration), with some individuals only developing clinical manifestations several years after leaving an endemic area.1,4,7,8 The overwhelming male predominance of the infection was highlighted in a recent review of 93 cases from
942 Infectious diseases of the skin
A
B
Mexico.9 One historic in vitro study revealed that 17β-estradiol inhibits or delays the transition of the fungus from its mycelial or conidial forms into pathogenic yeasts, thereby offering a plausible explanation for the relative rarity of the disease among women.10–12 Only 3% to 5% of cases occur in children and adolescents, who may present with acute or subacute disease.4,13
The natural habitat of the fungus remains an enigma.14,15 Natural infections have nevertheless been confirmed in nine-banded armadillos.14 It is assumed to be contracted via inhalation of conidia from soil contamination. The most common initial presentation is with pulmonary disease, which cavitates in 35% of cases.1,3 Primary lung infection, however, is often clinically silent. Involvement of the mucocutaneous junction in the nose and mouth occurs in approximately 65% of patients, whereas other skin sites are affected in only around 12% of cases.16 The most common other site is the face, where lesions may be ulcerative, verrucous, or crusted nodules.4
943 Coccidioidomycosis
Sarcoid-like facial lesions have also been described.17 Disseminated extrafacial lesions include erythematous or necrotic papules, pustules, ulcerated plaques, or even large nodules.18–23 Involvement of the external genitalia is exceptional.20,24 Primary lesions of the skin are very rare.5,13
A
Paracoccidioidomycosis is relatively uncommon in patients infected with HIV infection.8,19,25 A possible explanation for this is the fact that the disease tends to occur only in patients with advanced HIV/AIDS who are not receiving trimethoprim-sulfamethoxazole prophylaxis for P. jiroveci pneumonia, since this drug is also effective against P. brasiliensis.8 It has also been suggested that HIV/AIDS is a largely urban disease, whereas paracoccidioidomycosis tends to occur in more rural communities; the condition has nevertheless been documented occur among HIV-positive patients in endemic areas.13,25 The infection carries a 30% to 67% mortality in HIV/AIDS patients.26,27 Paracoccidioidomycosis has also been reported in patients with underlying Hodgkin lymphoma, non-Hodgkin lymphoma, or visceral neoplasms.18,28
B
There have been relatively recent reports of infection due to P. lutzii in the Midwest and Northern regions of Brazil. The clinical and epidemiological aspects of the aforementioned infection, however, have yet to be fully elucidated.5,29
Pathogenesis and histologic features The fungus P. brasiliensis is morphologically similar to B. dermatitidis, but P. brasiliensis has a thinner cell wall with a double contour appearance and produces multiple, narrow-based buds, said to resemble a ‘pilot’s wheel’.1 Mycelia from the dimorphic fungus produce conidia, which when inhaled into the lungs transform into pathogenic yeast forms.12 Although a genetic susceptibility to infection is suspected, no specific HLA antigen association has been confirmed thus far.12,30 Susceptible individuals may have a functionally deficient neutrophil response to the organism.31
confirmation of the infection in paraffin-embedded tissue specimens has been described.35 A real-time PCR method for rapid detection of the organisms in tissue biopsies also exists.7
Differential diagnosis Distinction from blastomycosis can be difficult, but P. brasiliensis does not have the multiple nuclei of B. dermatitidis and the budding pattern is quite different. Cryptococcus can show a similar variation in yeast size, but has its own characteristic mucicarmine-positive mucinous capsule and produces single buds.10,13
The histologic reaction to the infection in the skin resembles that of blastomycosis in that it is characterized by suppurative and granulomatous inflammation.10,13,31–33 Neutrophilic abscesses superimposed on pseudoepitheliomatous hyperplasia are seen. Eosinophils may be present in a high proportion of cases. Tuberculoid granulomas are encountered occasionally (Fig. 18.316).17,34 The budding yeast form is seen most often within multinucleate giant cells. The variably sized yeasts measure 2–20 µm in diameter, whereas the ‘pilot’s wheel’ has a diameter of up to 60 µm.10,13
The ‘pilot’s wheel’ appearance is diagnostic; however, if this is not seen, isolation of the organism in vitro is necessary to confirm the diagnosis. Mucosal reactions are similar to those seen in the skin. Transepidermal (transepithelial) elimination of the microorganism in association with spongiosis, microvesiculation, and microabscesses is commonly present.33 Scarring is a feature of older lesions. A case with associated necrotizing granulomatous arteritis has been reported.22 A PCR method for diagnostic

Fig. 18.311 Blastomycosis: (A) numerous ulcerated and crusted nodules are visible on the chest; the patient had systemic involvement. (B) There is severe facial involvement. Note the sepiginous border. (A) By courtesy of W. Weir, MD, Coppetts Wood Hospital, London, UK; (B) by courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.
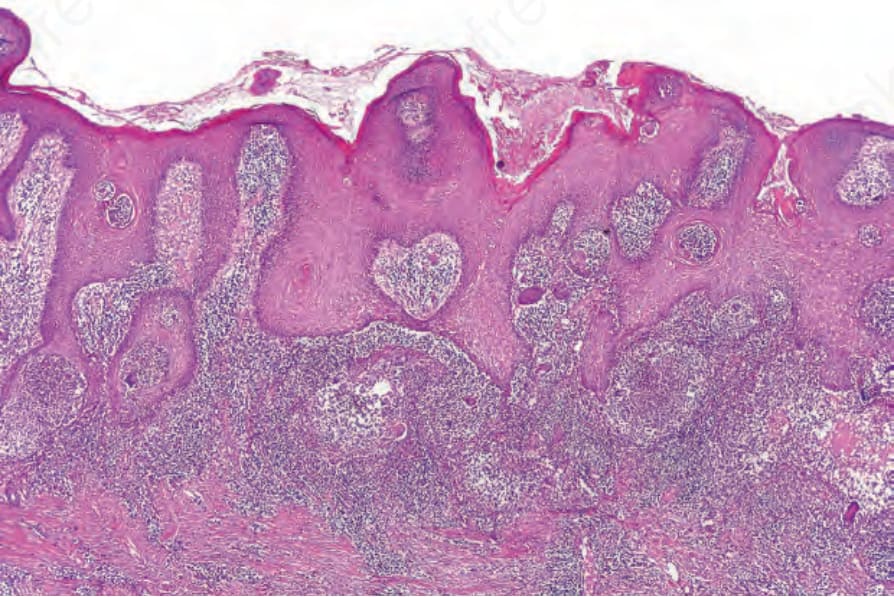
Fig. 18.312 Blastomycosis: there is massive pseudoepitheliomatous hyperplasia. Dermal abscesses and giant cells are evident.
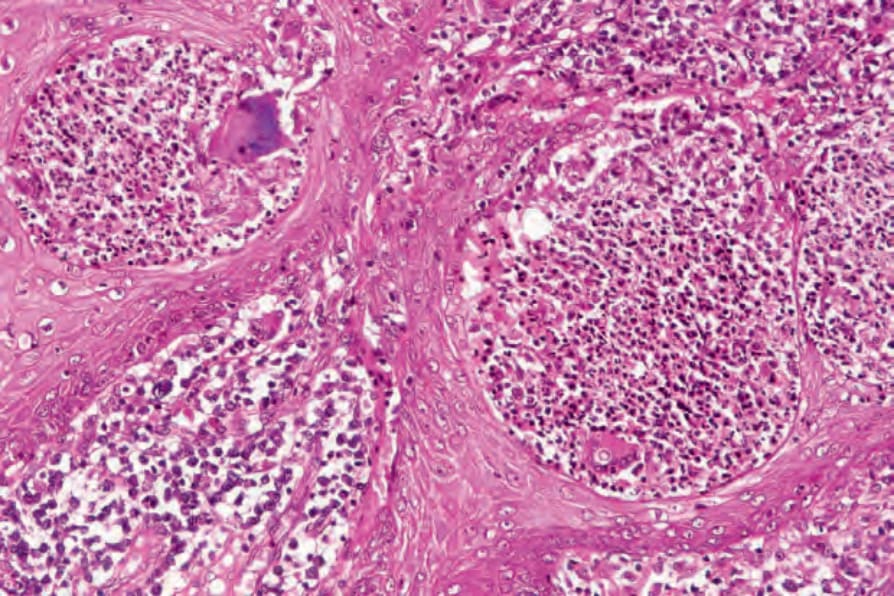
Fig. 18.313 Blastomycosis: close-up view showing mixed granulomatous and suppurative inflammation.
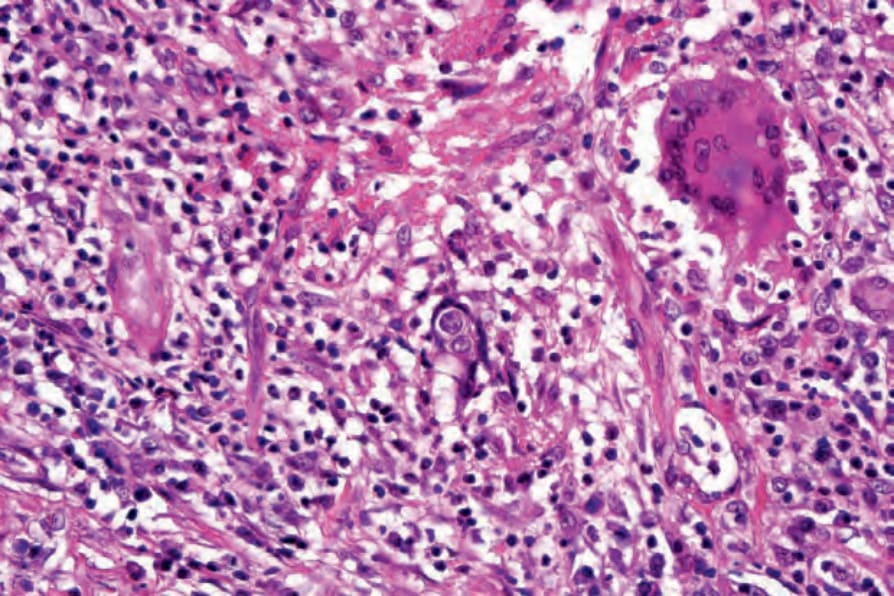
Fig. 18.314 Blastomycosis: note the characteristic broad-based budding and multiple nuclei.
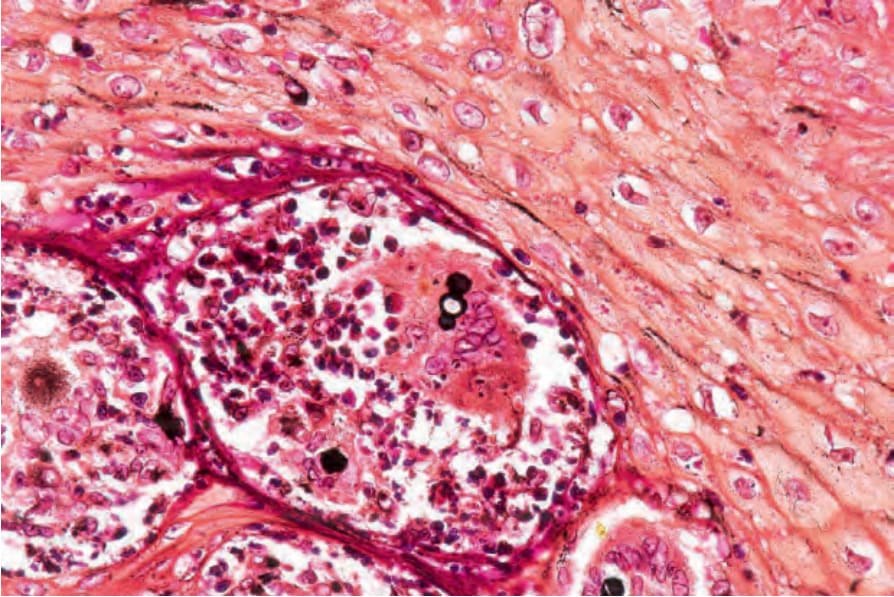
Fig. 18.315 Blastomycosis: silver stain showing broad-based budding.
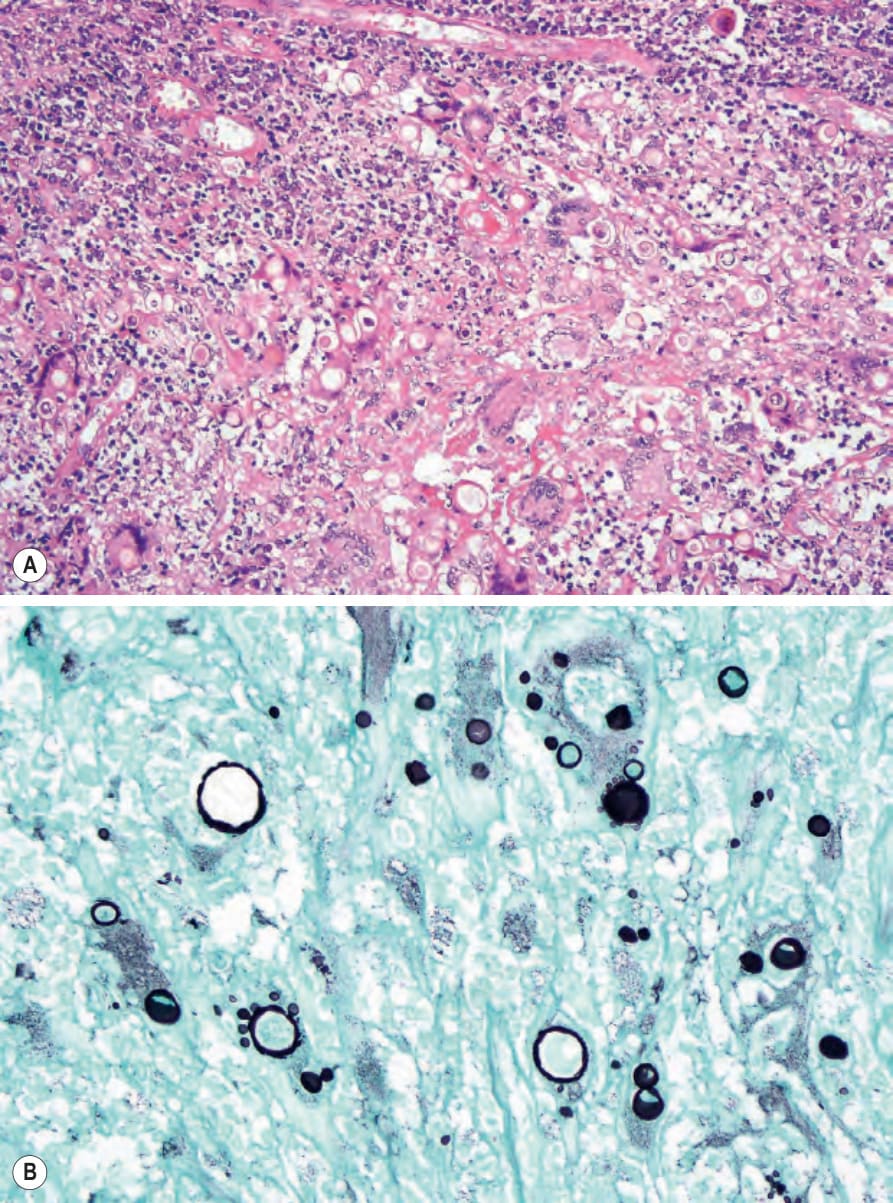
Fig. 18.316 Paracoccidioidomycosis: (A) numerous fungi are seen surrounded by granulomatous inflammation; (B) typical ‘pilot’s wheel’ budding is evident (methenamine silver). By courtesy of W. Robles, MD, Institute of Dermatology, London, UK.