Blastomycosis
Blastomycosis
Clinical features Blastomycosis (North American blastomycosis) is caused by Blastomyces dermatitidis. Although the soil is generally regarded as the usual habitat of this fungus, it probably also exists in wood and bird droppings. The infection was originally thought to be restricted to North America, but cases were subsequently reported in South America, Africa, India, and Israel.1–4 The organism is endemic in the states bordering the Mississippi and Ohio rivers, the Great Lakes, and the St. Lawrence Seaway.1,4–6 It has not yet presented as an endogenous disease in Europe or the Far East. Blastomycosis occurs most often in young to middle-aged adults and in males more frequently than in females.5,7 Although uncommon, the disease has been recorded in the pediatric population.8 The infection is most commonly acquired via the lungs after inhalation of airborne conidia, which occurs when moist soil
940 Infectious diseases of the skin
A
A
B
and organic debris containing the mycelia are disturbed.1,4,5,9 There are three clinical forms of the disease: pulmonary, disseminated, and primary cutaneous blastomycosis.
B
documented in iatrogenically immunosuppressed solid organ transplant recipients, in whom opportunistic co-infections may occur.13,14 In this clinical context, overall mortality may be as high as 67% if the pneumonia is complicated by acute respiratory distress syndrome.14
There is an incubation period of 33–44 days before the onset of respiratory symptoms, which are usually insidious. An acute pneumonic picture occurs, with potential progression to acute respiratory distress syndrome. The infection may also closely resemble tuberculosis both clinically and radiologically. Blastomycosis is not uncommonly associated with subclinical infection.1,4,10 In contrast to many of the other deep fungal infections mentioned in this chapter, blastomycosis most often develops in previously healthy hosts.7 A number of cases have nevertheless been documented in HIV-infected individuals, and although blastomycosis is not regarded as an AIDS-defining infection, certain clinical differences exist.11,12 CNS involvement is said to occur in 46% of patients, i.e., 5–10 times more frequently than in the HIV-negative population. Furthermore, the estimated mortality rate is five times that of non-HIV-infected patients with blastomycosis (54% vs. less than 10%).12 Although uncommon, the condition has been
The skin – in addition to bone, joints, CNS, and the genitourinary tract (prostatitis and epididymo-orchitis) – is usually involved following dissemination of a pulmonary infection.13,15 The lesions may be single or multiple and may affect any part of the body. The skin lesion starts as a papule, but gradually spreads and becomes an ulcerated and crusted, verrucous nodule or ulcerated plaque, with a serpiginous swollen red border (Fig. 18.311). This border extends, while the center may heal with scarring. Exuding pus is present beneath the peripheral crust. Rarely, a widespread pustular eruption may occur.16 These protean manifestations may lead to clinical confusion with keratoacanthoma, pyoderma gangrenosum, or panniculitis.10,17
Occasionally, primary cutaneous blastomycosis occurs 1–2 weeks after inoculation.18–20 This lesion starts as a pustule, which ulcerates superficially (chancre) and is associated with regional lymphadenitis, lymphadenopathy,
941 Paracoccidioidomycosis
A
A
B
B
and lymphangitic skin nodules, similar to sporotrichosis. Verrucous or fungating skin lesions are sometimes encountered.21,22 The condition may rarely present with isolated infection of the perianal skin.23 Chronic disseminated cutaneous blastomycosis has also been reported.24
Pathogenesis and histologic features B. dermatitidis is a thermally dimorphic fungus which exists in the yeast phase at 37°C in tissues. It grows as a mycelial form at 25°C. The yeasts are round, usually 8–15 µm, but occasionally up to 30 µm across, and have a refractile thick cell wall.8 They are multinucleate and produce single buds, which have a broad base.4,15,25 Infections with large yeast forms measuring 30–35 µm in diameter are an exceedingly uncommon occurrence.26 Microforms may also be encountered.25 The yeast forms of B. dermatitidis possess an adhesion-promoting protein termed WI-1 adhesin, which is thought to play a crucial pathogenetic role.27
and a panel of histochemical stains for infective microorganisms.25 Recognition of the fungi is facilitated by the use of PAS or methenamine silver stains (Fig. 18.315). The organisms also stain with Congo red.28
Differential diagnosis Distinction from other deep cutaneous fungal infections showing similar histologic features including chromoblastomycosis, coccidioidomycosis, paracoccidioidomycosis, and sporotrichosis rests on the absence of pigment and the presence of a characteristic multinucleate yeast form with single broad-based buds. In situ hybridization may provide a prompt diagnosis in those cases where tissue cultures are not obtained.29
The histologic features of blastomycosis include, in the early stages, a predominantly neutrophil infiltrate, and many organisms are seen. Subsequently, a granulomatous reaction develops in which multinucleate giant cells are numerous and neutrophils are still plentiful. The overlying epidermis shows striking pseudoepitheliomatous hyperplasia (especially in verrucous lesions), often containing numerous microabscesses (Figs 18.312 and 18.313).15,25 The Blastomyces organism is seen within giant cells and also free in the connective tissue (Fig. 18.314). A neutrophilic host response predominates in immunocompromised patients and those with a pustular form of the infection, emphasizing the need for both a high index of suspicion
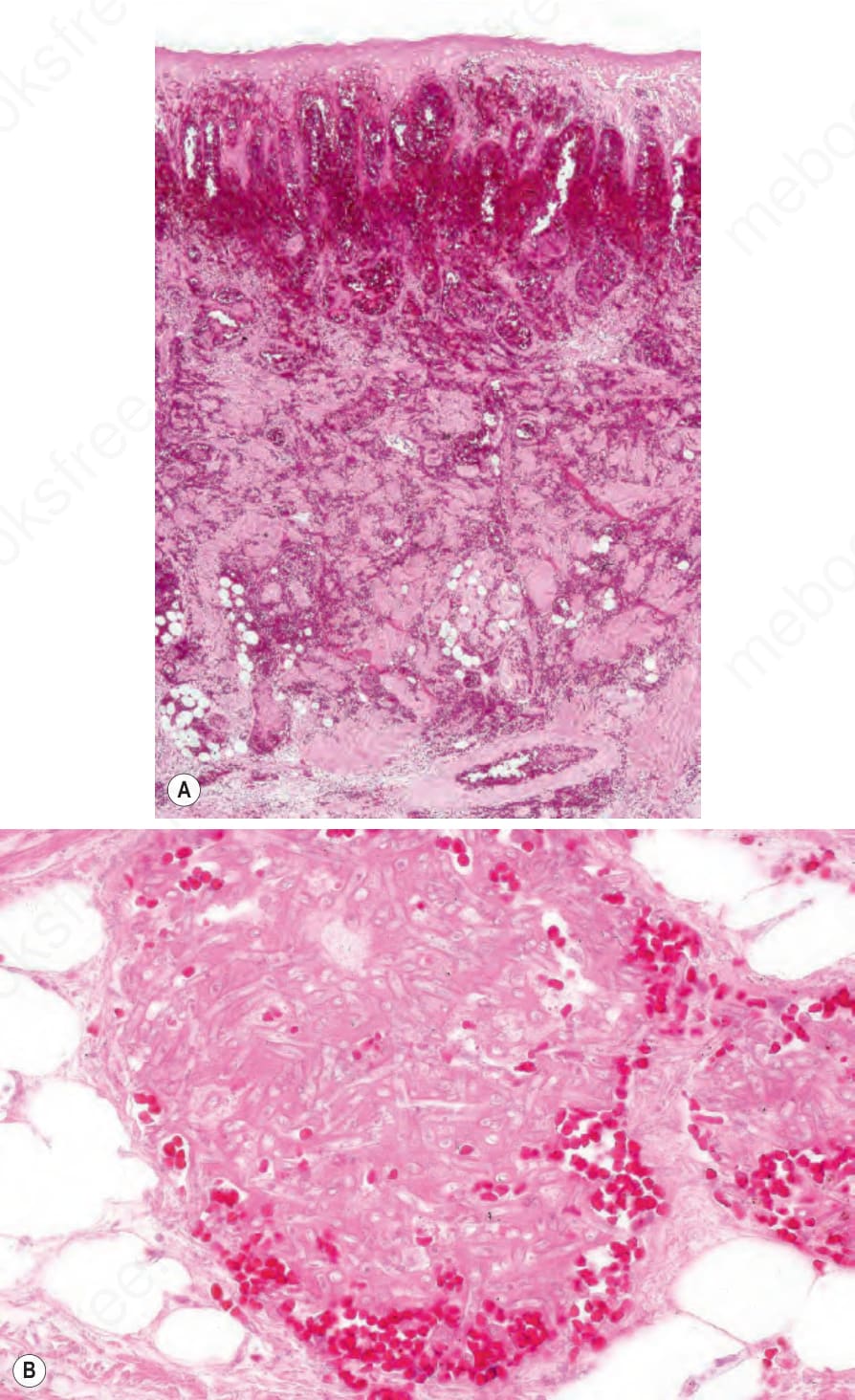
Fig. 18.307 Fusarium spp.: (A) low-power view showing epidermal infarction and massive hemorrhage; (B) note the thrombosed vessel containing numerous hyphae. By courtesy of A. Zembowitz, MD, Massachusetts General Hospital, Boston, USA.
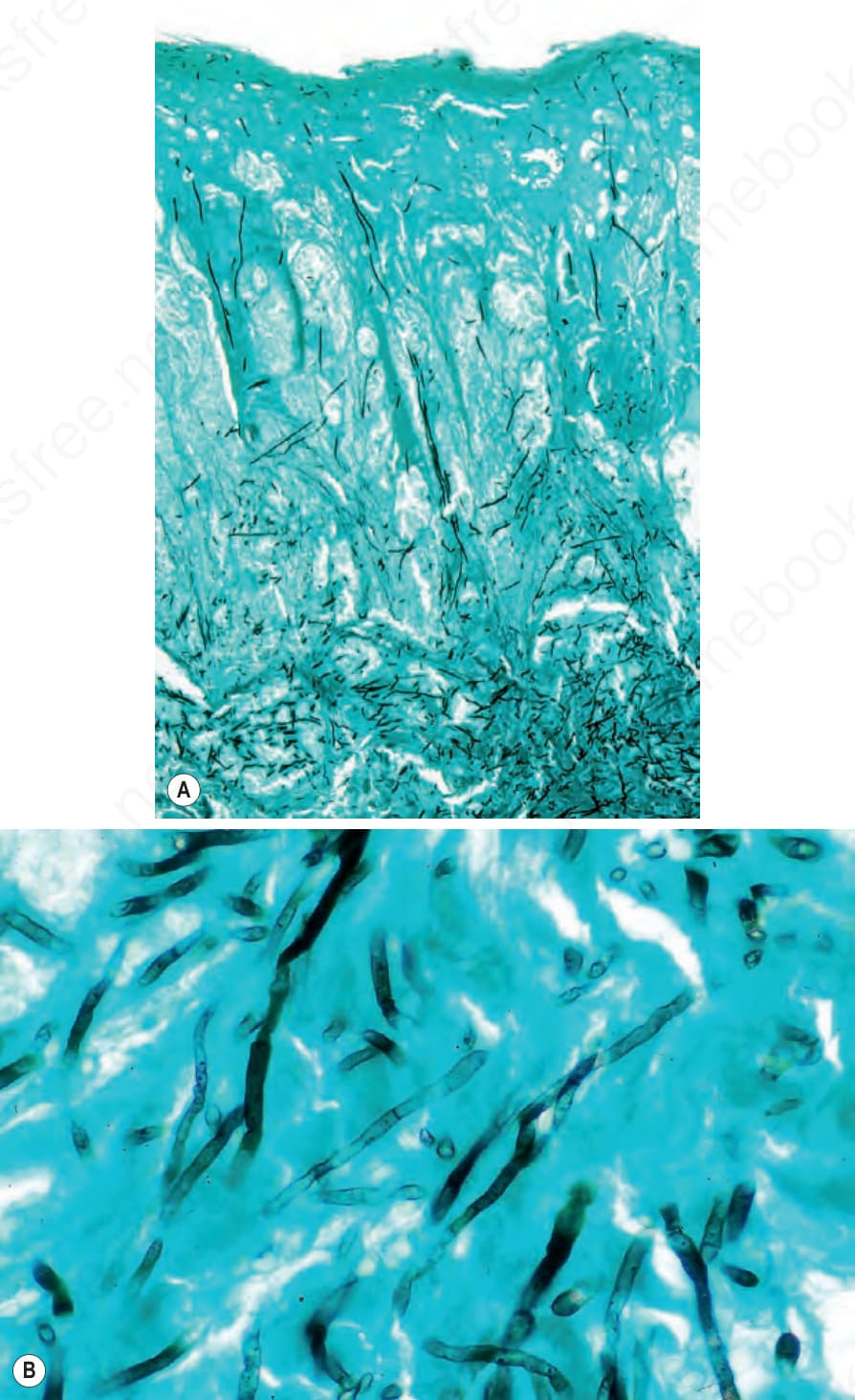
Fig. 18.308 Fusarium spp.: (A) hyphae extend from the deep dermis to the epidermis; (B) note the septa (methenamine silver). By courtesy of A. Zembowicz, MD, Massachusetts General Hospital, Boston, USA.
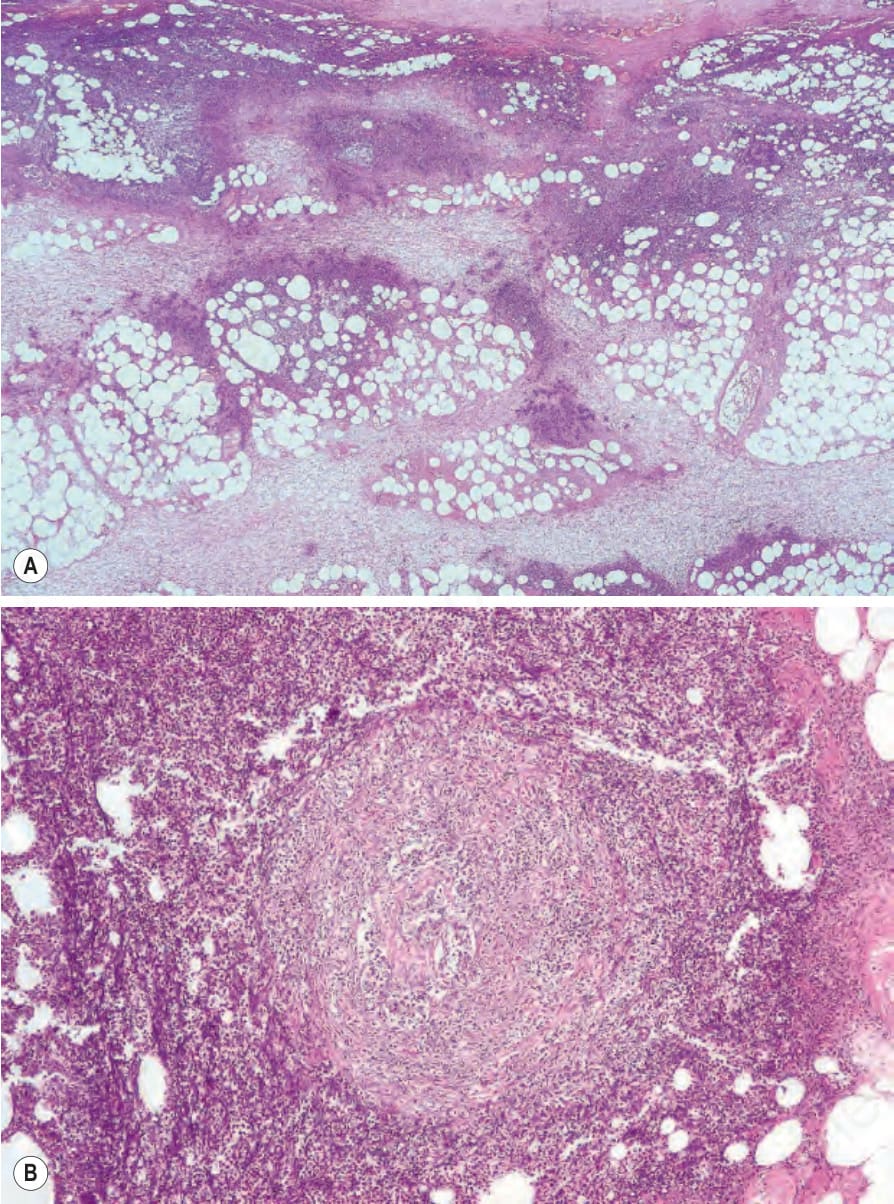
Fig. 18.309 Pseudallescheria boydii: (A) low-power view showing massive dermal inflammatory changes; (B) this field shows an inflamed and thrombosed vessel.
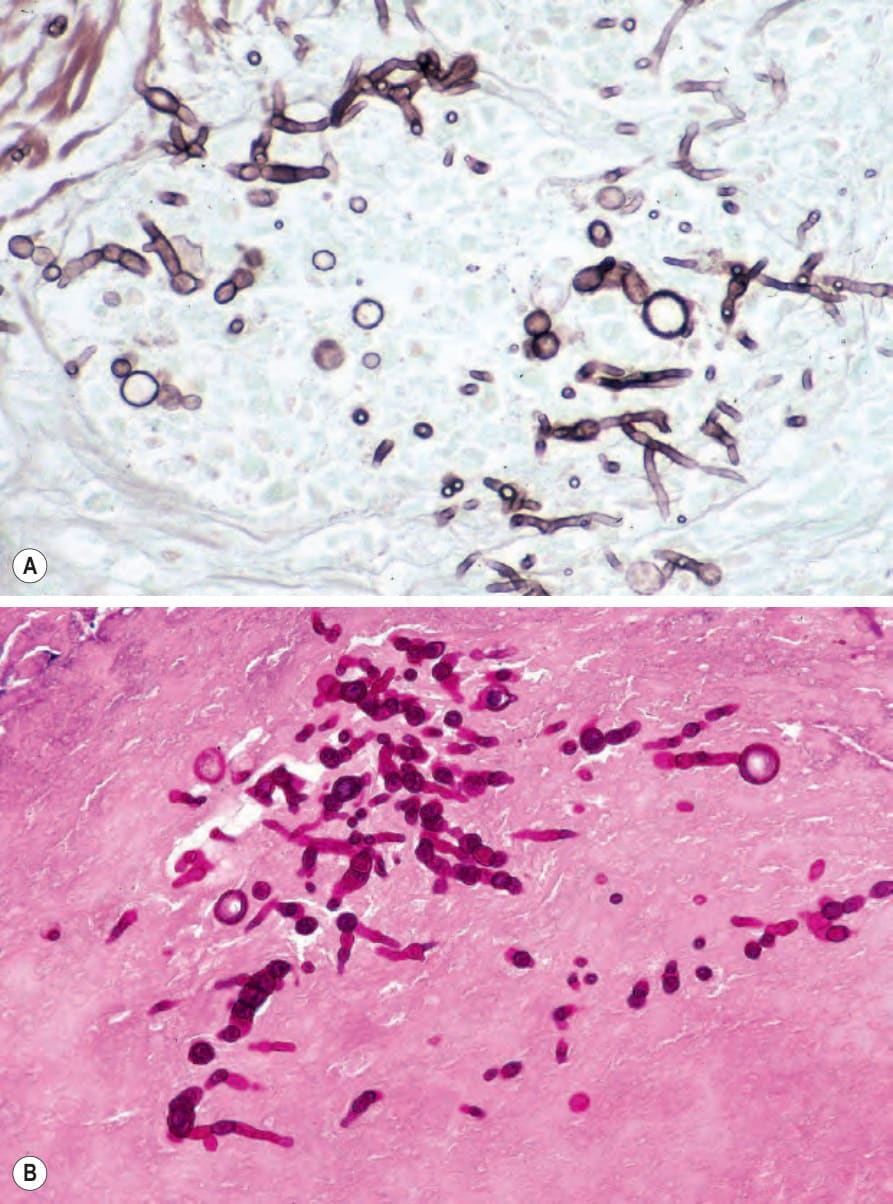
Fig. 18.310 Pseudallescheria boydii: (A) silver stain showing hyphae with chlamydoconidia; (B) periodic acid-Schiff stain.

Fig. 18.311 Blastomycosis: (A) numerous ulcerated and crusted nodules are visible on the chest; the patient had systemic involvement. (B) There is severe facial involvement. Note the sepiginous border. (A) By courtesy of W. Weir, MD, Coppetts Wood Hospital, London, UK; (B) by courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.
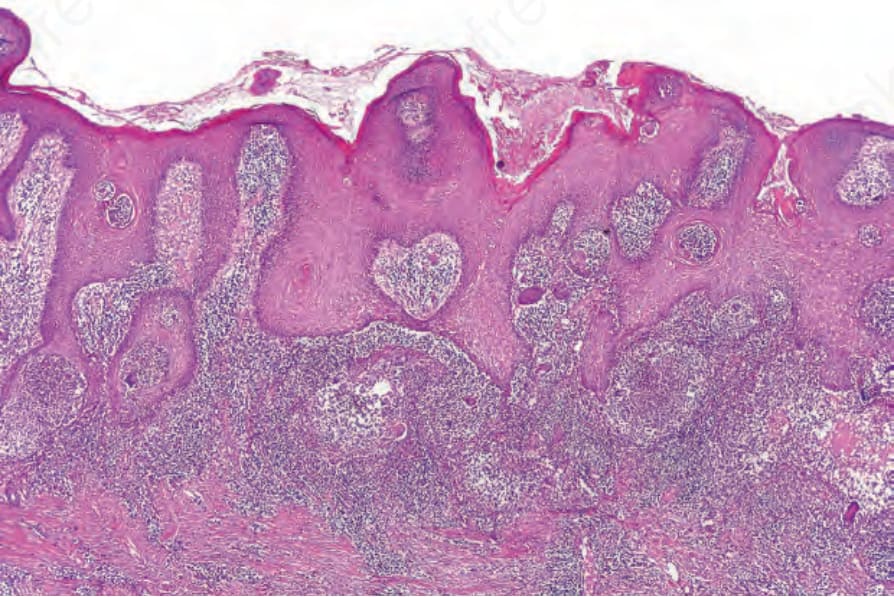
Fig. 18.312 Blastomycosis: there is massive pseudoepitheliomatous hyperplasia. Dermal abscesses and giant cells are evident.
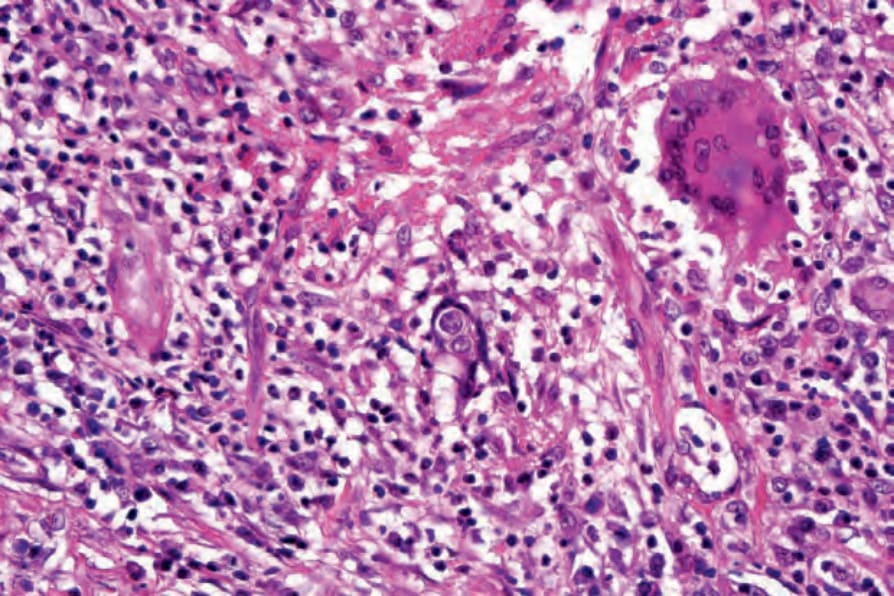
Fig. 18.314 Blastomycosis: note the characteristic broad-based budding and multiple nuclei.
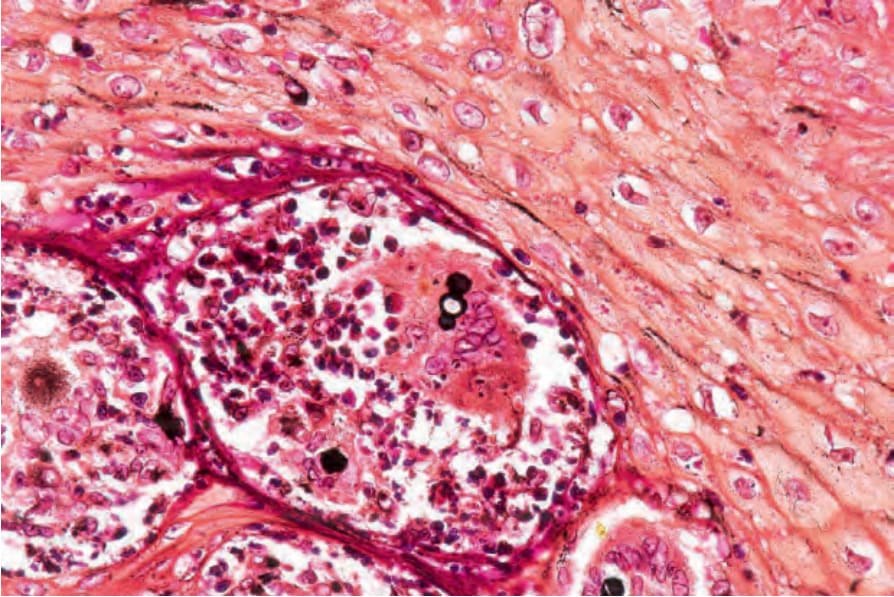
Fig. 18.315 Blastomycosis: silver stain showing broad-based budding.