Hyalohyphomycosis
Hyalohyphomycosis
Clinical features Hyalohyphomycosis is the generic term applied to fungal tissue infections caused by nondematiaceous, hyaline septate hyphal organisms.1–3 It generally does not encompass infections due to Aspergillus spp. and Penicillium spp., which are considered separately in this chapter. Members of the class Zygomycetes are specifically excluded from this category. The causative agents of hyalohyphomycosis include Fusarium spp., Pseudoallescheria boydii (and its asexual form, Scedosporium apiospermum), Acremonium spp., Paecillomyces spp., Trichoderma spp., Scopulariopsis brevicaulis.1–3 Hyalohyphomycosis has gained increasing relevance among immunosuppressed organ transplant recipients and patients with underlying hematological malignancies.3–5 A number of the aforementioned organisms also account for a small proportion of cases of onychomycosis.6,7
In the skin, the lesions form abscesses in the dermis, with central necrosis and pus, surrounded by granulomata.16 Eosinophils are sometimes numerous.18 The epidermis may occasionally exhibit pseudoepitheliomatous hyperplasia.18,24 The fungal elements, most commonly of A. fumigatus, are found in the necrotic center of the lesion. A. flavus, A. niger, A. glaucus, A. versicolor, A. nidulans, A. terreus, and A. tamarii represent additional etiological species.1,4,24,26,28,41–44 The infection may extend into the subcutis.40 Exceptionally, subcutaneous involvement may closely mimic pancreatic or gouty panniculitis, a phenomenon which has been ascribed to lipase production by the fungus.45
In cases of hematogenous spread, fungal hyphae may be identified within the lumen of thrombosed dermal blood vessels.20,46 The fungus is recognized by its uniform septate branching and radiating hyphae (with an arboreal growth pattern), with branches being equal in thickness (dichotomous) and at 45° (Figs 18.305 and 18.306).2,47 The hyphae are often not seen easily with H&E, but are well demonstrated by a silver stain, such as Gomori or Grocott.
Fusarium species (plant molds) are of increasing importance, particularly in immunosuppressed patients in whom they represent the second most common pathogenic mold.4,8–16 The most frequently encountered Fusarium species include F. solani, F. oxysporum, and F. moniliforme.3,13 Infections with F. veticillioides, F. petroliphilum, and F. proliferatum have also been reported.3,17,18 Patients can present with localized skin or soft tissue lesions, nail involvement, sinus infection, pulmonary fusariosis, or with disseminated disease.1–3,9,13,15,19 Risk factors for localized disease include trauma, burns, foreign bodies, stasis ulceration, penetrating plant injury, or iatrogenic cutaneous portals of entry.13,18,20,21 Systemic involvement occurs particularly in the setting of hematological malignancy and neutropenia, GVHD and corticosteroid therapy.8,9,12,13,15 Ulcerated, ecthyma-like, targetoid, or violaceous macular skin lesions may occur, while subcutaneous involvement manifests as multiple nodules.13,22–27 One unusual case presented initially with vesicular lesions following stem cell transplantation.28 In one study, superficial intertrigo-like skin lesions or nail involvement abnormalities due to colonization by Fusarium spp. was identified as a risk factor for the subsequent evolution of invasive fusariosis among high-risk patients with underlying hematological diseases.29 The reported mortality of disseminated fusariosis in immunocompromised hosts ranges from 50% to 80%.13,15,16,30
Differential diagnosis The fungus must be distinguished from other branching fungal infections, including the agents of hyalohyphomycosis (e.g., Fusarium spp., Pseudoallescheria boydii, Acremonium spp.) and the Zygomycetes. Distinction from the former, however, is not possible in routine histopathological sections, while the latter tend to stain well with H&E, consist of broader, twisted hyphae of variable thickness, and exhibit right angle branching. Diagnosis usually requires culture of the organism, but the finding of a fruiting head in tissue is confirmatory. Alternatively, a specific immunofluorescent antibody test, immunohistochemistry, or PCR techniques can be employed.2,47
939 Blastomycosis
transplant recipients.40,41 Localized infection of skin of the lower limb of an obese patient has been reported.39
A similar spectrum of disease may be encountered as a result of infection with Paecilomyces spp.2,42
Histologic features The various fungal genera responsible for hyalohyphomycosis cannot be distinguished from one another in routine histologic sections.43 More precise identification of the etiological agent, therefore, is reliant on fungal culture results and more recently, pan-fungal PCR involving amplification of among others, the internal transcribed spacer region.18 The latter molecular technique may also be applied to formalin-fixed, paraffin-embedded tissue samples. Routine histochemical stains such as PAS and methenamine silver aid in highlighting the contours of the hyphae and confirming the presence of septation.43
The histologic reaction in fusariosis varies from granulomatous to suppurative.44 In patients with disseminated disease, vascular involvement similar to aspergillosis is seen, including thrombosis of the involved vessels (Figs 18.307 and 18.308). The fungi present as hyaline, branching, septate hyphae measuring 3–8 µm in width.19 In contrast to Aspergillus, the hyphae branch irregularly, varying from acute-angled through to 90°.44 Fusarium spp. are capable of sporulating in tissues. Consequently, yeast-like structures can occasionally be seen in association with the hyphae.43 Fusarium sporodochia may rarely be encountered on infected traumatic cutaneous wounds.45
A
In immunosuppressed patients, P. boydii is most often encountered as an angioinvasive lesion similar to aspergillosis. The hyphae are septate, branching, hyaline, and measure 2–5 µm in width.46 They are histologically indistinguishable from Aspergillus spp. (Figs 18.309 and 18.310).
Differential diagnosis Infection with Aspergillus spp. constitutes the main differential diagnosis, as already alluded to above. Invasive candidiasis, which also has a propensity to occur in immunosuppressed and neutropenic patients and exhibits similar vascular involvement, can potentially be confused with hyalohyphomycosis in tissue sections, as the masses of elongated, overlapping pseudohyphae in the former can create the impression of branching. The pseudohyphae of Candida spp., however, are more slender, lack septation, and are accompanied by yeast forms measuring 3–5 µm in diameter.43
B
P. boydii and its asexual form, S. apiospermum, are also important causes of infection in the immunosuppressed, especially following solid organ transplantation and in the context of hematological disease.31–37 Diabetes mellitus and HIV/AIDS are further risk factors.3 Patients may also develop localized disease in the skin and subcutaneous fat including mycetoma.34,36 Clinical features in a large series of patients following organ transplantation included disseminated disease, skin lesions, lung disease, endophthalmitis, meningitis, brain abscess, mycotic aneurysm, and sinusitis.33 A sporotrichoid presentation has been described.31
The condition should also be distinguished from mucormycosis, another infection characterized by pronounced vascular invasion in susceptible individuals. The organisms associated with mucormycosis, however, are often better visualized in H&E-stained sections than those of hyalohyphomycosis, and comprise broader, twisted hyphae of variable thickness (7–15 µm or more in width), with right angle branching.47 Potential confusion with mucormycosis may nevertheless arise when the hyphae of hyalohyphomycotic species swell and assume a globose appearance.43 Correct identification of the causative organism, either by culture or with the aid of molecular mycology techniques, therefore, remains the final arbiter; this has implications for correct treatment.1–3
Acremonium spp. may be associated with onychomycosis, keratitis, infection of peritoneal dialysis fistulae, intracranial infections, prosthetic valve endocarditis, osteomyelitis, and mycetoma.2,7,38 Risk factors for invasive Acremonium infection include penetrating wounds, intravascular catheters, and underlying immunosuppression.39 Erythema nodosum-like tender subcutaneous nodules may occur on the legs, while multiple cutaneous and subcutaneous lesions are a feature of skin involvement as part of disseminated Acremonium infection in immunosuppressed patients, including organ
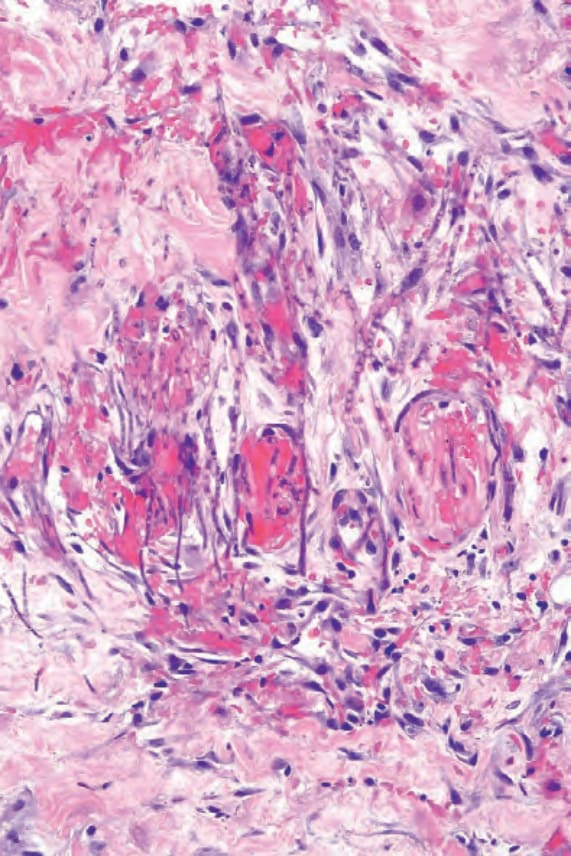
Fig. 18.305 Aspergillosis: high-power view showing vascular occlusion and fungal hyphae.
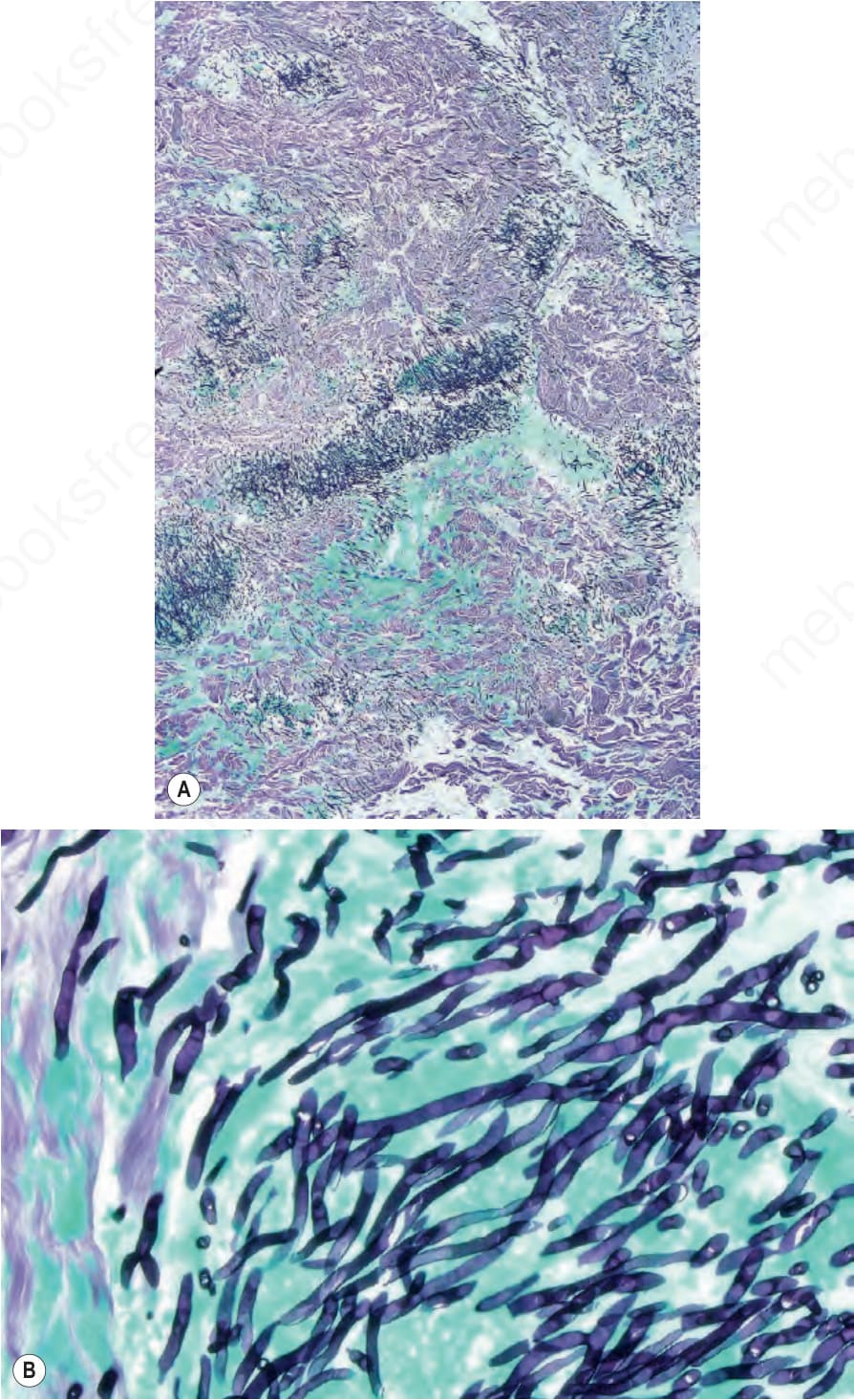
Fig. 18.306 Aspergillosis: (A) low-power view showing the massive infection and innumerable fungi emanating from the cutaneous vessels; (B) the hyphae are septate and branch at 45° (methenamine silver).
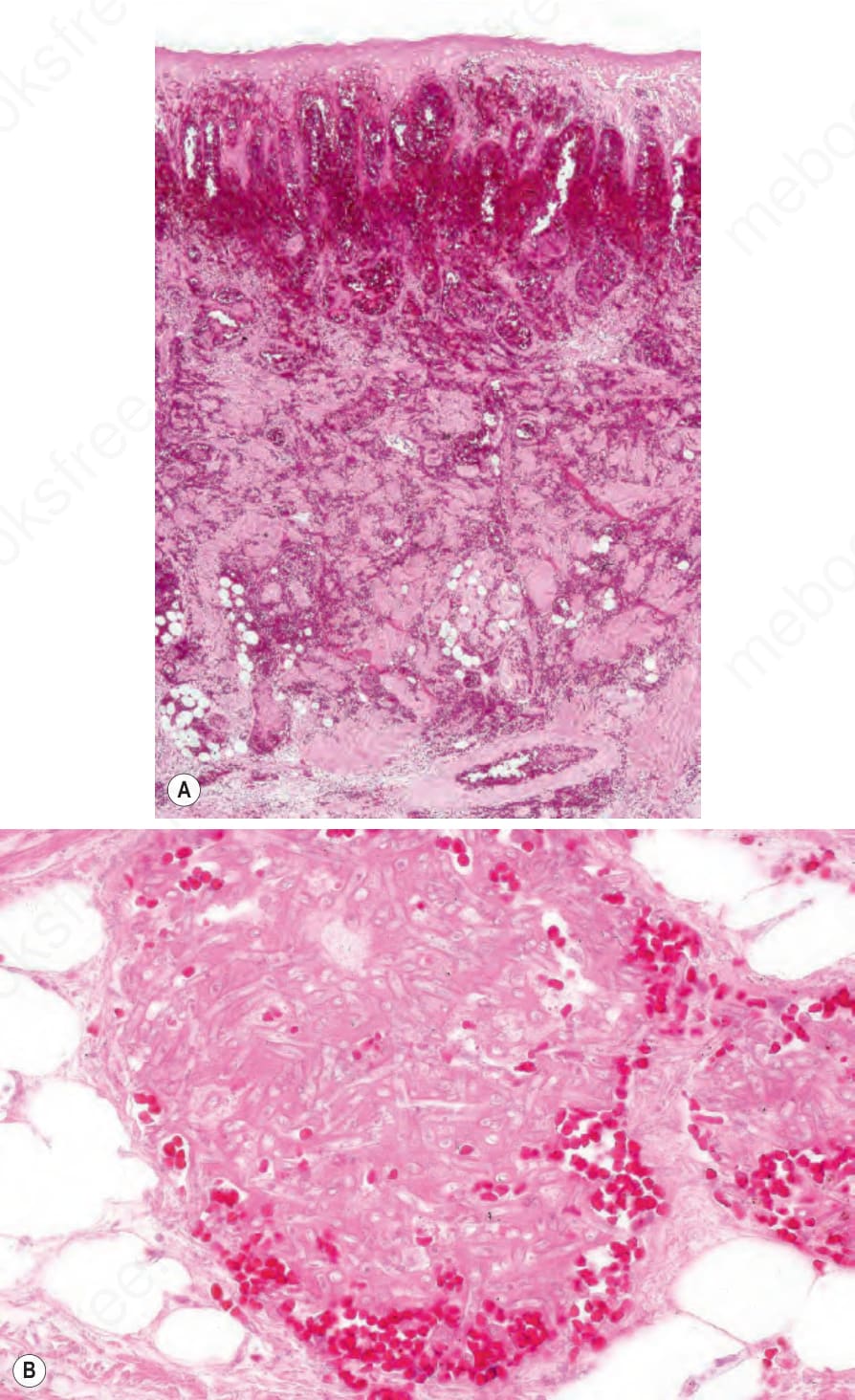
Fig. 18.307 Fusarium spp.: (A) low-power view showing epidermal infarction and massive hemorrhage; (B) note the thrombosed vessel containing numerous hyphae. By courtesy of A. Zembowitz, MD, Massachusetts General Hospital, Boston, USA.
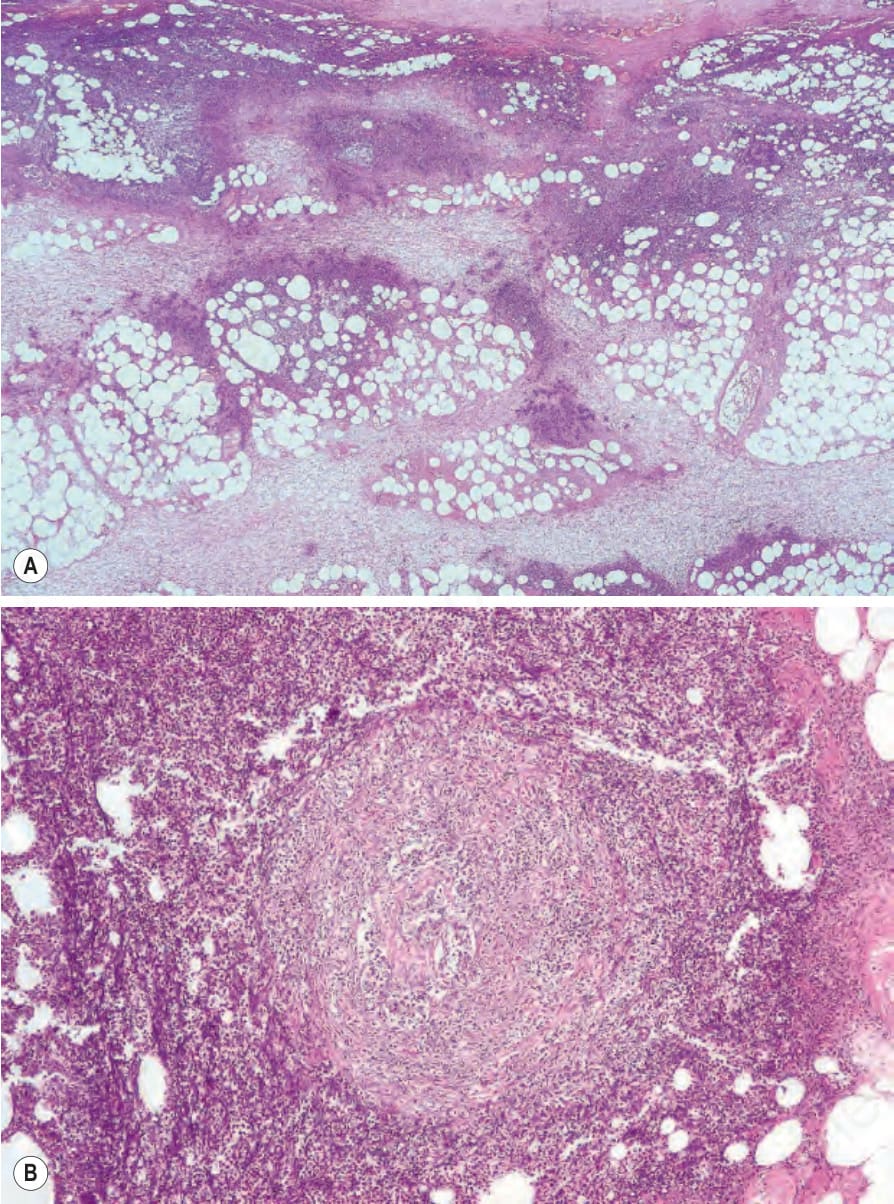
Fig. 18.309 Pseudallescheria boydii: (A) low-power view showing massive dermal inflammatory changes; (B) this field shows an inflamed and thrombosed vessel.