Aspergillosis
Aspergillosis
Clinical features Species of Aspergillus occur worldwide and can cause cutaneous lesions, either by hematogenous spread from a primary infection in an immunosuppressed patient, usually in the lung, or by direct inoculation of the skin.1–4 Aspergillus spp. are also a rare cause of onychomycosis.1,5,6 Patients with neutropenia are particularly at risk of systemic spread, especially those with hematological malignancies.4,7–11 Skin involvement secondary to disseminated aspergillosis has also been reported in the context of HIV/AIDS, diabetes mellitus, following bone marrow transplantation, in extremely low birth weight preterm neonates, and in a child with underlying chronic granulomatous disease.11–16 Patients may develop widespread pulmonary infiltrates or infarction, which is soon followed by disseminated vaso-occlusive disease.3,17 Systemic lesions are most commonly seen in the gastrointestinal tract, the CNS, the liver, kidney, heart, and thyroid.9 Destructive lesions of the palate and nasal septum may occur.1,18 Skin involvement in disseminated aspergillosis is uncommon, however, being present in only about 4% to 5% of patients.7,19 Less than 1% of patients in a recently reported series of 1410 cases of invasive aspergillosis had cutaneous lesions secondary to systemic involvement.20 In hematogenous spread, the lesions develop as small, red, discrete macules and papules, which may become pustular or necrotic/ infarcted (Fig. 18.302). Plaques studded with pustules may be seen. Noduloulcerative lesions with central eschar formation and raised borders are sometimes encountered.18,20 Very rarely, a tumorlike mass may develop.16
Primary aspergillosis of the skin, which usually follows local trauma (e.g., intravenous injection therapy site, cutaneous maceration, or burns), appears as a purplish thickened edematous area at the site of inoculation.21–28 Infection has also been described following a home-made tattoo.29 In the immunosuppressed, these lesions may ulcerate and develop a black crust (Fig. 18.303).19,20,30 A presentation mimicking Sweet syndrome has been reported.31 The condition has also been reported in premature infants and those with underlying HIV/AIDS.23,32–36 Occasional immunosuppressed patients with primary cutaneous aspergillosis have presented with solitary nonulcerated nodules.37,38 Multiple nodules may also occur in these patients.39,40 On rare occasions, however, even immunocompetent individuals may develop multiple nodular lesions and plaques.41 There is a report
of evolution of large cauliflower-like lesions on the legs of a patient with bilateral postfilarial elephantiasis.42
All lesions of aspergillosis are commoner in the immunosuppressed, and the outcome follows the progress of the immune status. In general, however, the infection is often rapidly fatal due to visceral involvement.1,10,21 Patients receiving corticosteroid therapy appear to be particularly susceptible to the development of cutaneous aspergillosis.4,21 A recently published review of factors influencing patient outcome in primary cutaneous aspergillosis revealed an 18.5% rate of dissemination and a mortality of 31.5% among susceptible immunocompromised individuals.36
938 Infectious diseases of the skin
Pathogenesis and histologic features Aspergillus is ubiquitous in the environment and inhabits soil and organic debris so that pulmonary lesions are found in farmers and gardeners (Fig. 18.304). It can contaminate grain and affect birds. It is often present in public buildings, including hospitals, due to contamination of air vents and central heating plants by bird droppings. Despite the wide distribution of the fungus, infection usually requires previous immunosuppression, as in patients receiving corticosteroids or who have lymphoma or leukemia. The host response to the mycelial component of the infection is the neutrophil, whereas the conidia forms are phagocytosed and killed by macrophages. Both lines of cellular response need to be deficient for the infection to become progressive. The production of fungal toxins also assists the establishment of infection.2,3

Fig. 18.302 Aspergillosis: this immunosuppressed patient developed multiple purple nodules on the limbs secondary to esophageal candidiasis. By courtesy of A.F. Nascimento, MD, Brigham and Women’s Hospital and Harvard Medical School, Boston, USA.

Fig. 18.303 Aspergillosis: there is extensive ulceration with characteristic black crusting. Primary cutaneous aspergillosis most often follows trauma or it may develop in the immunosuppressed. By courtesy of N. Khardori, MD, University of South Illinois, USA.
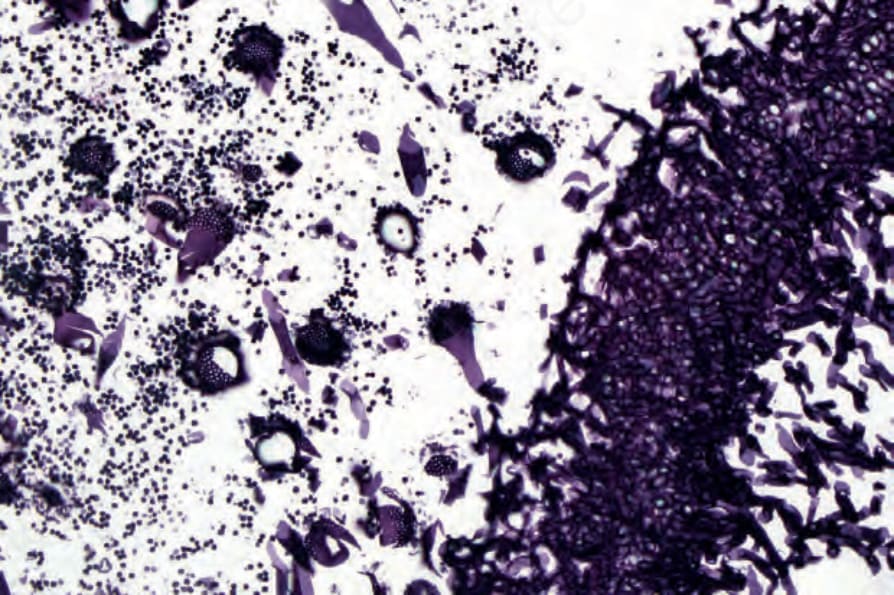
Fig. 18.304 Aspergillosis: the fruiting head (aspergillum) as shown in this picture is formed when the fungus is exposed to air. It is not usually seen in the tissues. Methenamine silver stain. By courtesy of R. Margolis, MD, St Elizabeth’s Medical Center, Boston, USA.
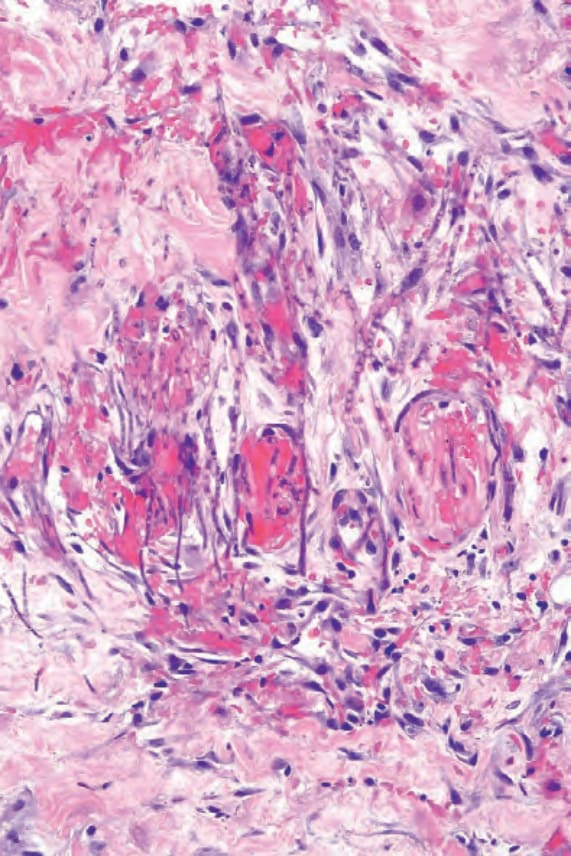
Fig. 18.305 Aspergillosis: high-power view showing vascular occlusion and fungal hyphae.