Candidiasis
Candidiasis
Clinical features Candida is a yeast-like fungus with budding and filamentous (pseudohyphal and hyphal) forms. There are several species, but C. albicans is by far the most common human pathogen.1,2 C. glabrata (formerly Torulopsis glabrata) infections, however, have become increasingly important in recent years, especially in immunosuppressed hosts.3–5 C. parapsilosis and C. tropicalis are the next most frequently encountered pathogens; the former has been shown to proliferate in glucose-containing pareneteral solutions and is an important nosocomial pathogen, especially among low birth weight neonates.2,6,7 C. dubliniensis has emerged as a cause of oral candidiasis in HIV-infected patients.8 Other less frequently encountered species are C. guilliermondi, C. lusitaniae, C.orthopsilosis, C. metapsilosis, C. kefyr, and C. krusei.2,6,9–11 Some of the aforementioned non-albicans species of Candida are intrinsically resistant to certain antifungal agents.2,9,12
Candida infection involving mucocutaneous sites can be categorized as follows: oral candidiasis, cutaneous candidiasis, candidal vulvovaginitis, candidal balanitis, chronic mucocutaneous candidiasis (CMC), subcutaneous candidal abscess, and disseminated candidiasis.
Oral candidiasis appears in several forms13:
• In neonates, it appears as a curdlike pseudomembrane overlying an erythematous base, which may be painful and atrophic.
• In adults, usually males, a chronic hyperplastic form is seen as a plaque with an erythematous margin (Fig. 18.293). This must be distinguished from leukoplakia. This hyperplastic plaquelike form also occurs in the chronic mucocutaneous forms of candidiasis and in immunodeficient individuals, including those with HIV/AIDS.14,15
• Chronic atrophic candidiasis is seen in the elderly, often as a sore red patch associated with dentures. It may be accompanied by angular
cheilitis and sometimes extends onto the facial skin as an erythematous granular lesion. Candidal cheilitis may affect the lips of patients with a heavy oral candidal infection (Fig. 18.294). Steroid therapy, whether local or systemic, appears to predispose to oral involvement. Cutaneous candidiasis tends to be confined to skin folds in the obese and to the genital mucous membranes (Fig. 18.295). The lesions appear as moist erythematous areas with small pustules at the margins (Fig. 18.296). A variant of cutaneous candidiasis referred to as ‘decubital candidosis’ has been described in chronically bedridden patients and is invariably attributable to infection with C. albicans.16 Congenital cutaneous candidiasis is a very rare, self-limiting form of cutaneous candidiasis in which neonates present with a generalized erythematous papular eruption secondary to
935 Candidiasis
underlying Candida chorioamnionitis and funisitis.17,18 This latter condition must be distinguished from skin involvement as part of disseminated congenital candidiasis (see below).
Vulvovaginitis occurs mainly during pregnancy or as a complication of diabetes mellitus, oral contraceptives, or antibiotic therapy.2
Candidal balanitis is associated with vaginal infections in the sexual partner: transient papules develop on the glans, become white and pustular, and rupture; they may heal rapidly or persist with exacerbations (Fig. 18.297).
CMC is a persistent and refractory condition, usually starting in the young and often associated with an immunodeficient state. These patients have oral candidiasis, which recurs after therapy and may become hypertrophic. They also have cutaneous candidiasis involving intertriginous areas and the face and hands or in a more widespread distribution. Paronychia and vulvovaginitis or balanitis also occur (Fig. 18.298). CMC is also an important feature of HIV/AIDS.14 Indeed, oral candidiasis may represent an early marker of immunosuppression in patients with HIV infection.15 Candida vaginitis is an important early manifestation in female HIV/AIDS patients.14
936 Infectious diseases of the skin
A
Some of these patients have a severe congenital primary defect of cellular immunity, such as hereditary thymic dysplasia or the DiGeorge syndrome, and in these patients the outlook is poor (Fig. 18.299). Recent evidence has shown that impaired IL-17 immunity plays a key role not only in certain syndromic forms of CMC, but also in individuals who develop mucocutaneous candidiasis following IL-17 blockade as a result of targeted immunotherapy.19–21 Autosomal recessive autoimmune polyendocrinopathy syndrome (also referred to as autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy syndrome) is a rare disorder caused by mutations in the autoimmune regulator gene (AIRE) and the production of neutralizing autoantibodies against IL-17. In addition to CMC, patients may present with endocrinopathies involving the parathyroids, thyroid and/or adrenals, diabetes mellitus, nail dystrophy, and dystrophy of the dental enamel. Additional stigmata can include vitiligo, alopecia areata, and alopecia totalis.20,22–26 Patients with this condition may have altered patterns of cytokine production in response to infection by Candida organisms.25 Autosomal dominant hyper-IgE syndrome is another condition associated with syndromic CMC; the latter is a consequence of impaired generation of IL-17-producing Th17 cells, usually due to mutations in the STAT3 gene.20,21,27
B
Subcutaneous candidal abscess is a rare condition that is usually encountered in immunocompromised patients. Lesions may arise following iatrogenic intervention, such as central venous catheterization.28 There are isolated reports of severe necrotizing soft tissue infections caused by Candida spp., namely, NF and Fournier gangrene.29,30
In patients with HIV/AIDS and others who are immunosuppressed, such as severely neutropenic oncology patients, disseminated candidiasis follows hematogenous spread from an underlying gastrointestinal or urinary tract primary focus of infection. Candidemia is associated with a very high mortality rate.31,32 Cutaneous lesions include macules, papules, plaques, petechiae, hemorrhagic foci, nodules, and an ecthyma gangrenosum-like presentation. These are painful, multiple, and widely distributed over the body.32,33 A rare congenital form of disseminated candidiasis has been described, including very low birth weight infants.34,35 Disseminated disease may also be seen in heroin addicts. Candidemia and disseminated candidiasis are important infections in the nosocomial setting, especially among critically ill patients in intensive care units. Risk factors include invasive procedures (e.g., insertion of central venous catheters), parenteral nutrition, use of broad-spectrum antibiotics, the administration of corticosteroids, and renal insufficiency. There has also been a shifting trend toward infections with non-albicans Candida spp. in this context, with an accompanying increase in mortality and resistance to antifungal agents.12,36
Pathogenesis and histologic features
C. albicans and other Candida spp. have a number of virulence factors that potentiate infection. These factors include adhesins (which facilitate adhesion to epithelial surfaces), aspartyl protease (which facilitates penetration of keratinized cells), hydrolases, and phospholipases.7,37–40 In addition, the organisms utilize at least two signaling pathways that potentiate conversion from a yeast form to a hyphal form; the latter is a prerequisite for deeper penetration into keratinized epithelium.37,40,41 Additional attributes contributing to virulence include biofilm formation and phenotypic switching.7,40
Candidal lesions appear similar in varying sites. There is a prominent neutrophil infiltrate of the oral mucosa or epidermis. Yeast forms, pseudohyphae, or even true hyphae can be seen (Fig. 18.300). The yeast-like form is often seen in the mouth and does not necessarily indicate pathogenicity. There is often an intense chronic inflammatory infiltrate in the underlying connective tissue, and in chronic hypertrophic forms the epithelium is hyperplastic and hyperkeratotic.
The disseminated lesions are characterized by a fibrinous exudate with both yeast and pseudohyphae forms, sometimes accompanied by the features of a leukocytoclastic vasculitis. Vascular involvement may be associated with epidermal necrosis and vesiculation. Transepidermal elimination of organisms is a rare finding.32 Suppurative folliculitis and perifolliculitis are seen in heroin addicts.42 A recently reported case of disseminated C. krusei infection in a hematopoietic stem cell transplant recipient with fatal relapse of acute myeloid leukemia also demonstrated striking folliculocentricity; the
937 Aspergillosis
latter was attributed to apparent transfollicular elimination of organisms following clearance of the fungemia.11
The closely related species C. glabrata (formerly Torulopsis glabrata) differs from C. albicans by the general absence of hyphae and pseudohyphae in the former, although this is not always the case (Fig. 18.301).43
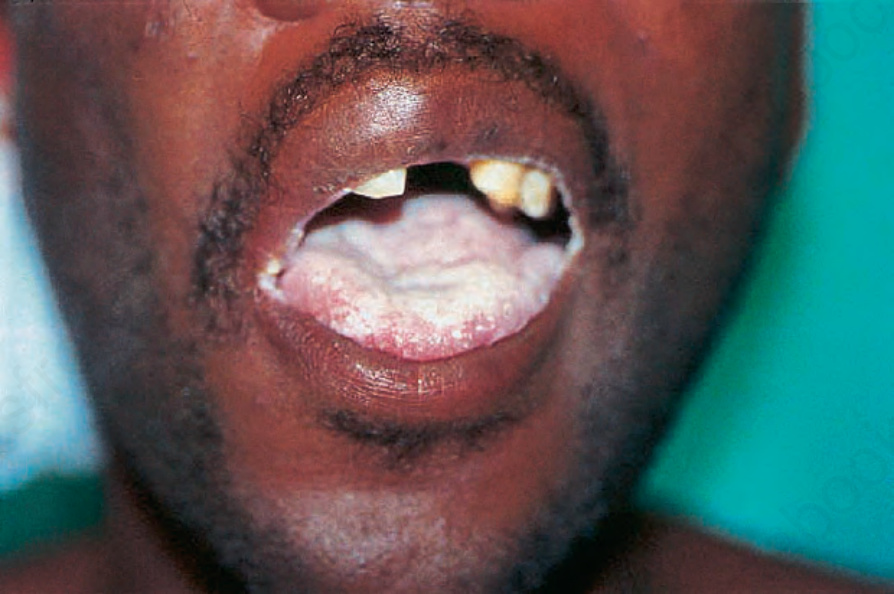
Fig. 18.293 Candida glossitis: the tongue is covered with a white plaque. There is also involvement of the angles of the mouth. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.

Fig. 18.294 Candidal angular cheilitis: note the erythematous crusted lesions at the angles of the mouth. By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.

Fig. 18.295 Cutaneous candidiasis: the warm, moist environment of the upper thighs and scrotum predisposes to intertriginous candidiasis. Note the erythema and peripheral pustules. By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.

Fig. 18.296 Cutaneous candidiasis: intertriginous involvement may be characterized by the development of pustules, as seen in this picture. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 18.297 Candidal balanitis: note the erythema with erosion and the small white pustule at the margin of the lesion. By courtesy of C. Furlonge, MD, Port of Spain, Trinidad.

Fig. 18.298 Candida infection: there is proximal nail dystrophy and onycholysis with pigmentary changes. By courtesy of the Institute of Dermatology, London, UK.

Fig. 18.299 Disseminated candidiasis: disseminated disease in infants may be a sign of immunosuppression such as DiGeorge syndrome. By courtesy of the Institute of Dermatology, London, UK.
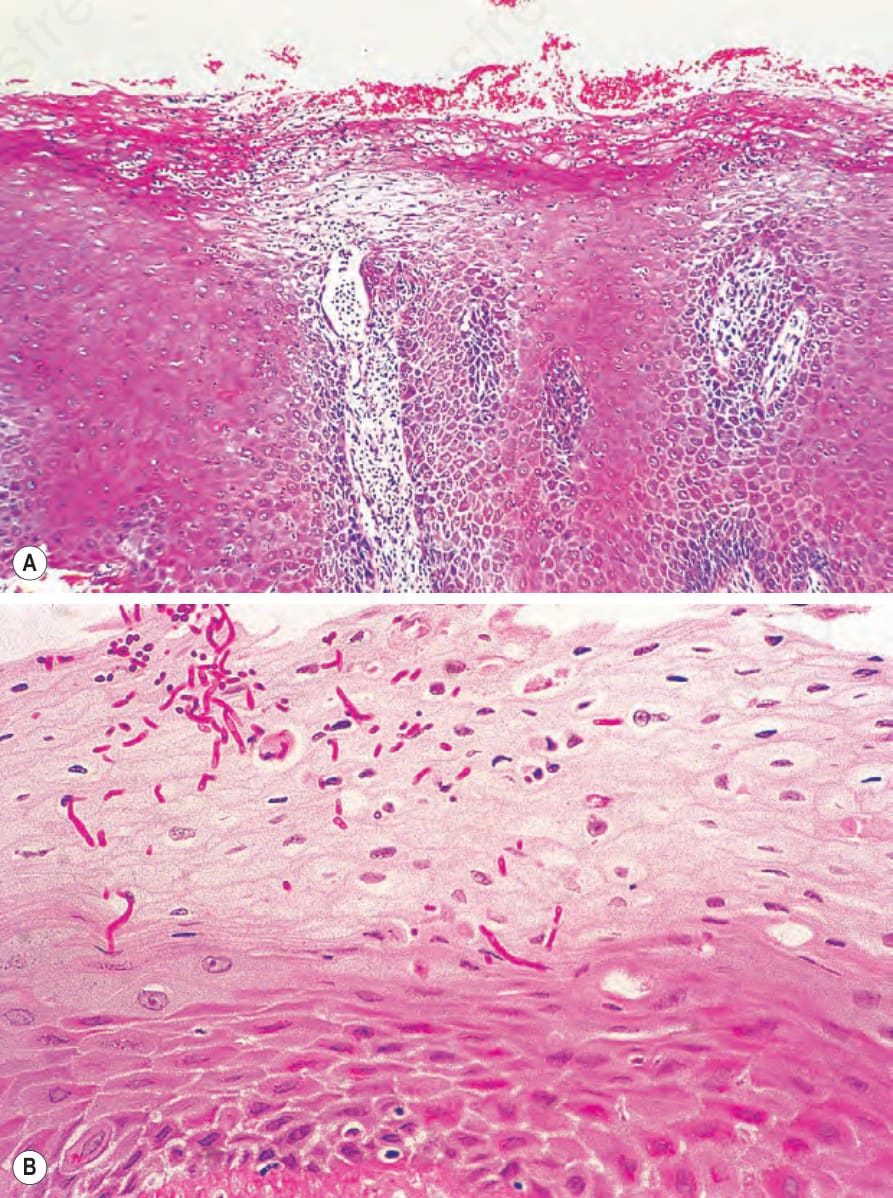
Fig. 18.300 Cutaneous candidiasis: (A) there is marked acanthosis and the superficial layers of the epithelium are infiltrated by large numbers of neutrophils; (B) there are abundant yeast-like and pseudohyphal forms (periodic acid-Schiff).
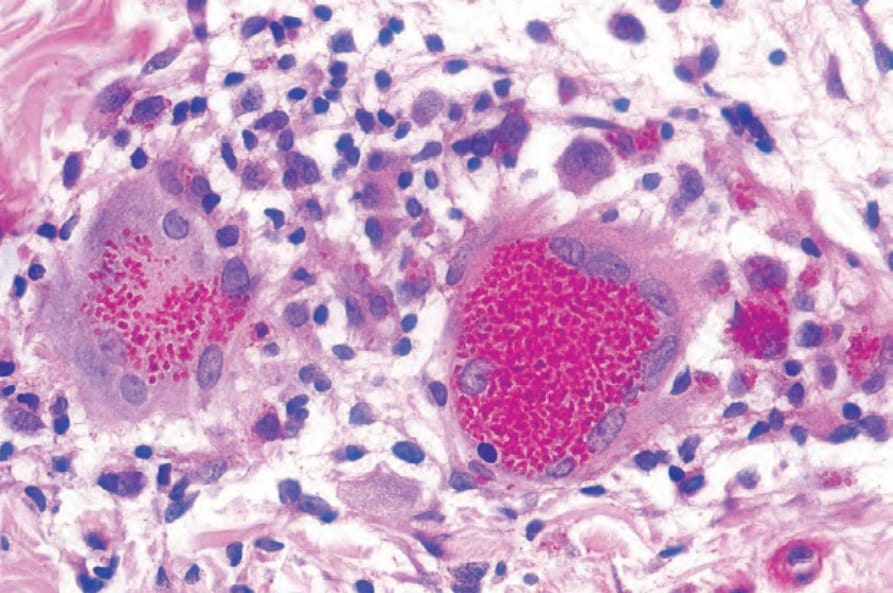
Fig. 18.301 Candida glabrata infection: intracytoplasmic location of the yeasts an uncommon manifestation.