Malassezia folliculitis
Malassezia folliculitis
Clinical features Malassezia folliculitis, which is often still referred to by its previous name, Pityrosporum folliculitis, is a form of chronic folliculitis attributed to infection by the yeast phase of M. furfur (formerly Pityrosporum ovale or P. orbiculare), an organism that thrives in hot, humid, and sweaty environments.1–4 The condition occurs in adults, who present with pruritic pustules centered mainly on the trunk, neck, and upper arms (Fig. 18.291). The disease has some propensity to occur in immunocompromised hosts and those on prolonged therapy with broad-spectrum antibiotics, and is an uncommon cause of pruritic papulopustular eruption in HIV-infected individuals.2,5–7 Malassezia spp. have also been linked to catheter-related fungemia in immunocompromised patients.5
with pigment-laden macrophages in the upper dermis. Greater numbers of yeasts and hyphae are present in hyperpigmented lesions.13 Biopsies from atrophic lesions may reveal variable epidermal and dermal atrophy with effacement of rete ridges, superficial dermal fibrosis, pigmentary incontinence, and elastolysis.15,16
The mechanism for the changes in pigmentation is not yet fully understood. Over the years, racial factors, light exposure, the inflammatory response, the fungal load, the thickness of the keratin layer, and a direct effect of the fungus (dicarboxylic acids) on melanocytes have been suggested.13,20–24 A multifactorial pathogenesis, however, seems likely, with a complex interplay between fungal wall constituents, enzymes, metabolites, and cellular components of the epidermis.25 Exposure to sunlight has been shown to stimulate the production of azelaic acid, and this is believed to lead to evolution of the hypopigmented lesions.26 Dopa cell counts have been shown to be normal.13 In hypopigmented lesions, there appear to be reduced numbers of smaller melanosomes in both the melanocytes and their neighboring keratinocytes.13 Mitochondrial and cytoplasmic vacuolation has also been documented. In the superficial dermis, a slight perivascular chronic inflammatory cell infiltrate consisting of lymphocytes, histiocytes, and occasional plasma cells may be evident.
Pathogenesis and histologic features Follicular occlusion may be the initiating pathogenetic event.8
Histopathological examination shows distension of occluded hair follicle infundibula by basophilic keratinous debris containing clusters of round, budding yeast cells (Fig. 18.292). Mycelial forms are characteristically absent. A mild perifollicular mononuclear inflammatory cell infiltrate is usually observed. Intradermal rupture of dilated follicles may incite an intense folliculocentric suppurative inflammatory infiltrate and perifollicular foreign body giant cell reaction. A PAS stain may reveal rare yeasts in the inflamed perifollicular dermis in such cases. Intrafollicular mucin deposition has been reported.9
There is also evidence to suggest that infection with the fungus rarely presents as systemic illness and that it is of importance in the pathogenesis of some cases of chronic folliculitis (Malassezia folliculitis, see below) and seborrheic dermatitis.1,6,9,12,19,27–29
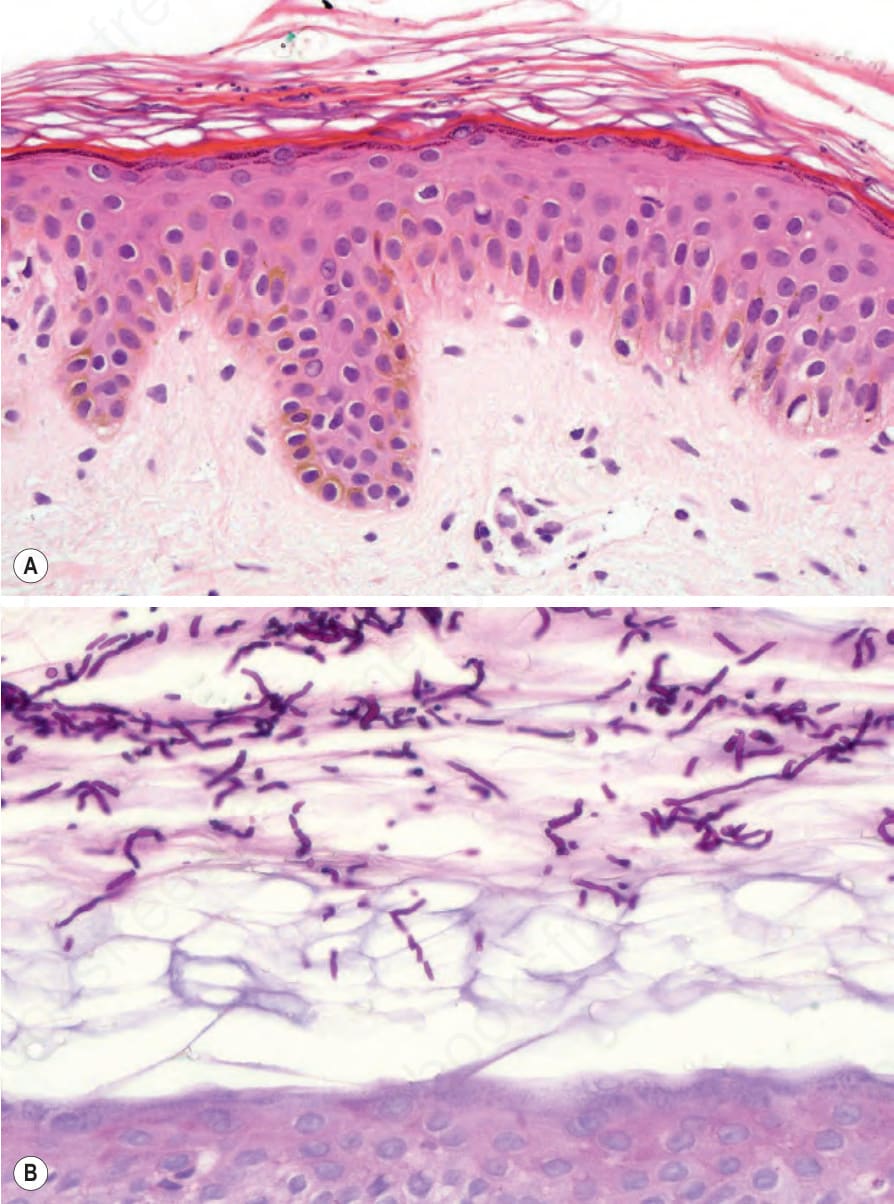
Fig. 18.290 Tinea versicolor: (A) there is hyperkeratosis and small basophilic spores are easily seen; (B) the periodic acid-Schiff reaction reveals numerous hyphae.

Fig. 18.291 Malassezia (Pityrosporum) folliculitis: note the numerous follicular pustules. By courtesy of S. Glassman, MD, University of Witwatersrand, Johannesburg, South Africa.
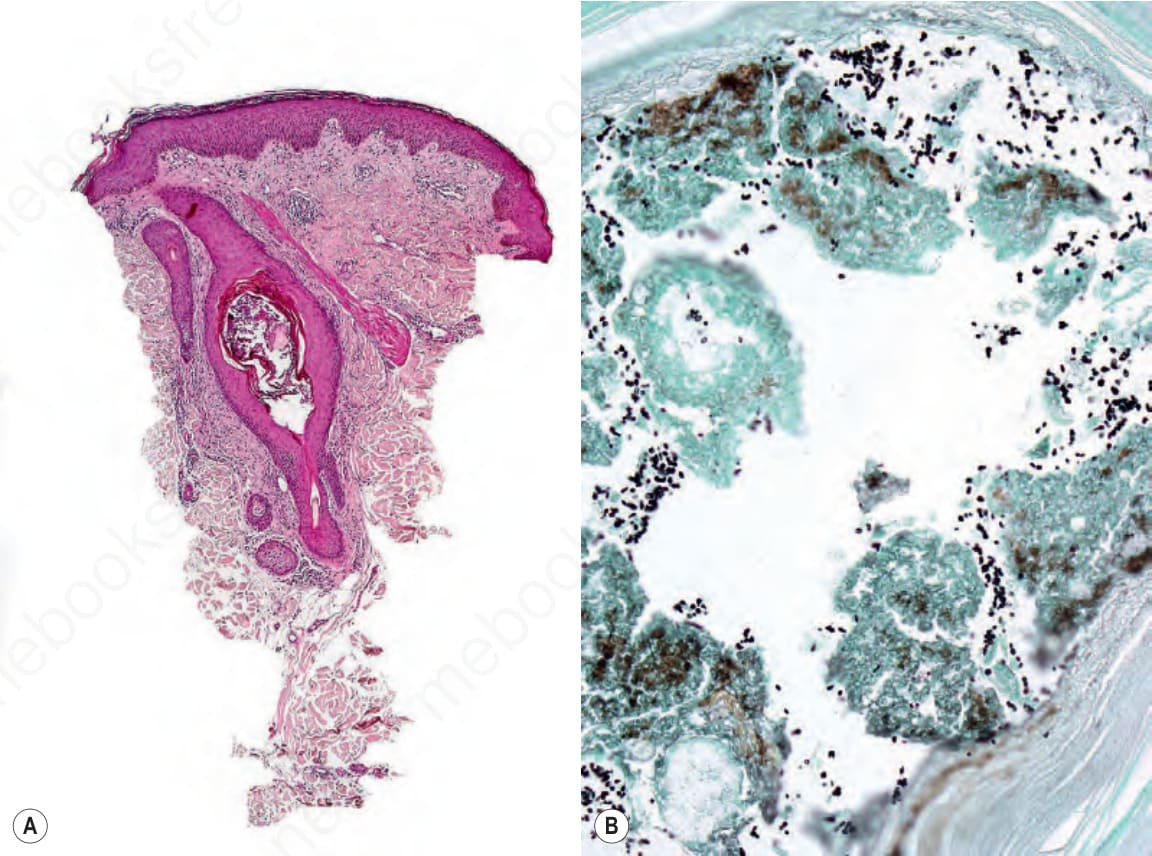
Fig. 18.292 Malassezia (Pityrosporum) folliculitis: (A) there is infundibular dilatation; (B) yeast forms are conspicuous in the methenamine silver stained section.