Toxoplasmosis
Toxoplasmosis
Clinical features Toxoplasmosis is the result of infection with Toxoplasma gondii, an obligate intracellular parasite.1 Infection in humans, who serve as the intermediate host, usually occurs following ingestion of T. gondii oocysts that are present in the feces of infected cats, or via consumption of undercooked, contaminated meat containing tissue cysts. The oocysts and tissue cysts then transform into tachyzoites, which in turn develop into bradyzoites after localization in brain or muscle tissue. These slowly replicating forms are contained within pseudocysts in the involved tissues.1,2
Differential diagnosis Acanthamebiasis and balamuthiasis are distinguished from cutaneous infection with E. histolytica by the presence of erythrophagocytosis in the latter
The zoonosis exists in a number of clinical forms: as an acute infection in immunocompetent individuals, the vast majority of whom are asymptomatic; congenital toxoplasmosis due to transplacental spread of a maternal infection, forming part of the TORCH group of infections; and acute disease in immunocompromised hosts, which is either acquired or the result of reactivation of latent infection.1,3 Although fever, lymphadenopathy, chorioretinitis, and cerebral involvement are well-recognized manifestations of symptomatic toxoplasmosis in general, presentation with skin lesions is uncommon. Cutaneous involvement is encountered more frequently in immunocompromised patients with disseminated infection, such as those with HIV/AIDS or in immunosuppressed recipients of bone marrow, hematopoietic, or solid organ transplants.1,4–15 Toxoplasmosis-associated hemophagocytic syndrome has been reported in a renal allograft recipient.16 The disease has also occurred following chemotherapy for lymphoma.11
Skin manifestations of the disease are very rare but may be encountered in cases of acquired or congenital toxoplasmosis.17 Potential dermatological manifestations include a maculopapular skin rash, widespread purpuric papules and nodules, thrombocytopenic purpura, lichenoid and erythema multiforme-like eruptions, ulcerative and vegetating lesions, panniculitis, and erythroderma.8,9,11–13,18–22 A case with vesicular lesions resembling varicella has also been reported.14
A
Histologic features A majority of reported cases have shown a superficial and deep perivascular inflammatory cell infiltrate composed of lymphocytes and histiocytes.4,18,20 Small ‘cysts’ containing tiny bradyzoites may be encountered in the dermis, including vascular endothelial cells, follicular epithelium, and the sweat glands and their ducts (Fig. 18.256).8 Rarely, similar structures are observed in the epidermis.9,13 The organisms may be highlighted by staining tissue sections with the May-Grünwald-Giemsa method.18 Free parasites are sometimes haphazardly distributed in the dermis, and there may be dermal edema, erythrocytic extravasation, necrobiotic collagen bundle, and karyorrhectic debris.8 Biopsies from severely immunocompromised patients may reveal little by way of a host response.8 Interface dermatitis and panniculitis have been described.10,11,15 One reported case presenting with erythroderma showed features of exfoliative dermatitis, with no discernible organisms.21 Vegetating lesions are characterized by pseudoepitheliomatous hyperplasia, sometimes accompanied by necrosis.18 Nodular lesions harbor macrophages whose cytoplasm contains bradyzoites.12 The diagnosis may be confirmed by ultrastructural examination, immunohistochemistry, or PCR.8,9,11,13,14
B
Differential diagnosis Cutaneous toxoplasmosis should be distinguished from histoplasmosis and leishmaniasis. Toxoplasma bradyzoites may potentially be mistaken for the intracellular yeast forms and amastigotes usually contained within macrophages in the aforementioned conditions, respectively. Leishmania organisms have a discernible kinetoplast. Rare cases of cutaneous toxoplasmosis following hematopoietic stem cell transplantation may mimic interface dermatitis, resulting in confusion with an adverse drug reaction or graft-versushost disease if the encysted bradyzoites are overlooked.10,15
923 Protothecosis
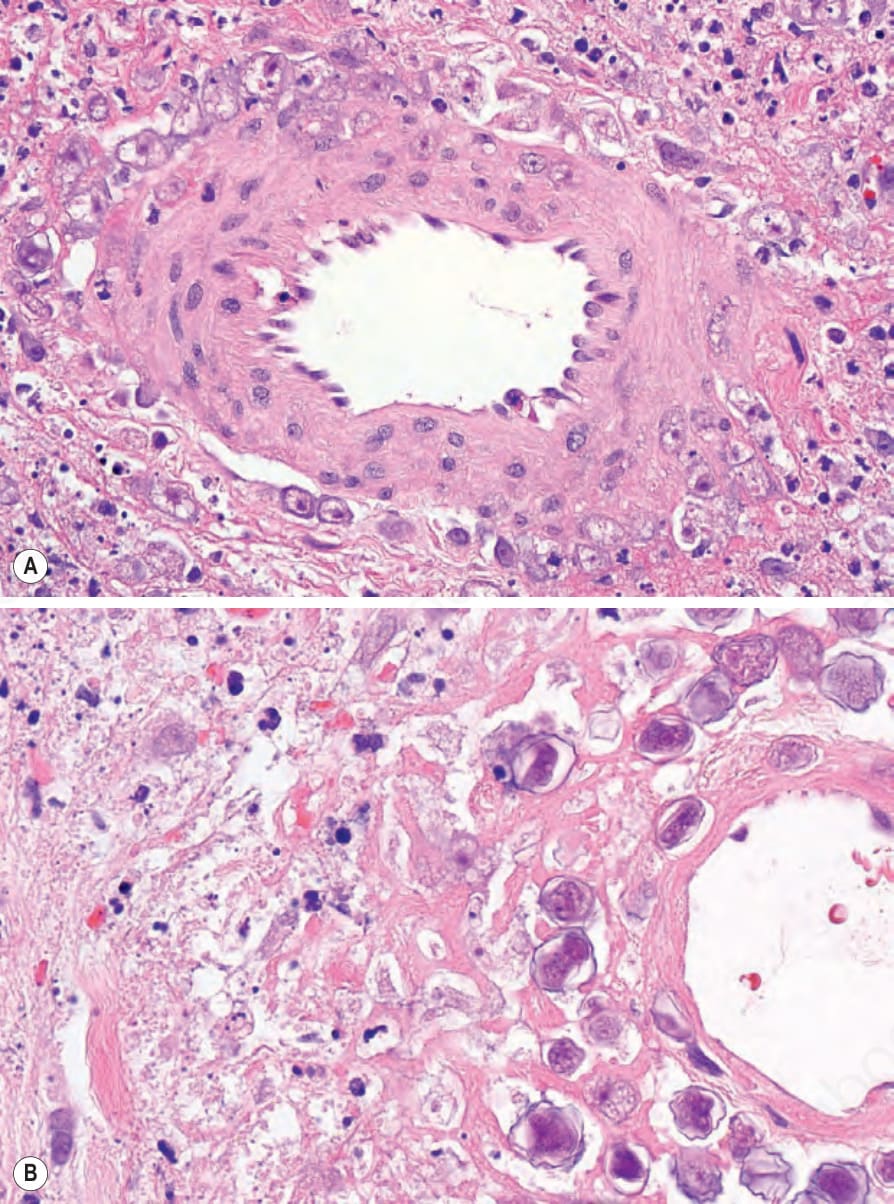
Fig. 18.255 (A, B) Acanthamebiasis: trophozoites and cysts are present. The wall of the latter is characteristically double layered (B).
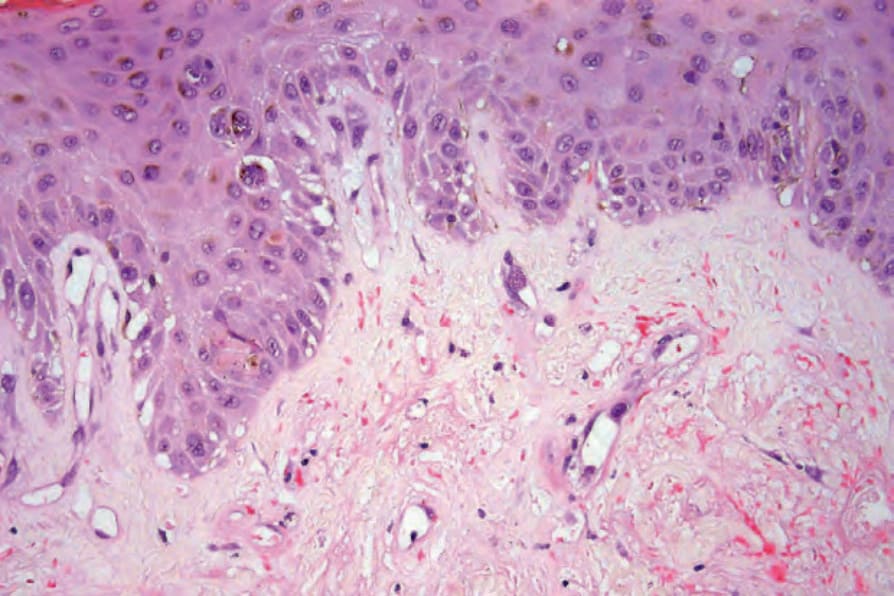
Fig. 18.256 Toxoplasmosis: a cyst containing numerous bradyzoites is present within a superficial blood vessel. By courtesy of H. Diwan, MD, Baylor College of Medicine, Houston, Texas, USA.