Amebiasis cutis
Amebiasis cutis
Clinical features Entamoeba histolytica can cause cutaneous lesions, although this is rare.1–3 Although some authors include infections by free-living amebae (i.e., Acanthamoeba spp. and Balamuthia mandrillaris) under the umbrella of cutaneous amebiasis, these latter infections are discussed separately in this chapter; use of the term amebiasis cutis will thus be restricted to E. histolytica infection in this section.
Amebiasis cutis is most commonly seen after surgical treatment of intestinal or hepatic amebiasis, but may also occur by direct extension perianally from the bowel or from hepatic involvement, and by direct inoculation of the skin from other infected lesions. A number of cases have been recorded in HIV-infected patients, who may have an increased mortality due to other co-infections.1,3–5 The infection may be sexually transmitted. Penile amebiasis, for example, can follow anal intercourse.6,7 Cutaneous lesions have been recorded on the trunk, abdominal wall, buttocks, genitalia, and perineum, and on the legs.1,4,6–11 In addition to ulcers, cutaneous amebiasis may present with fistulae, fissures, abscesses, and polypoid or warty lesions.1 Subcutaneous swellings called amebomas have also been described.12 Primary disease is uncommon; the majority of patients develop contiguous skin lesions in the presence of underlying visceral infection.1,3,5,13 Although the condition is encountered mainly in adults, amebiasis cutis may sometimes occur in children.2,3,9,14,15 A male preponderance of almost 2:1 was observed in a Mexican series of 26 cases.3
measuring from 1.5 × 2.5 to 4.5 × 6.8 µm.8 They appear blue-gray on H&E staining. A small rod-like similarly stained kinetoplast may be visible (Fig. 18.252). Many of the organisms are within macrophages, but some occur extracellularly. They are termed Leishman-Donovan bodies.14 These features must be distinguished from the similar bodies of histoplasmosis and, to a lesser extent, those of granuloma inguinale and rhinoscleroma. The clinical features will usually be distinctive; skin testing, serology, and culture of the organisms will confirm the diagnosis. PCR is useful in providing a rapid diagnosis with precise species identification.19,20,59,60
The lesions have a central necrotic zone with a purulent exudate, gray slough, an undermined margin, and an erythematous halo. The ulcers are irregular but sharply defined. They spread and do not heal spontaneously. They are extremely painful and may be destructive. Occasionally, the lesions resemble ulcerating tumors and are associated with surrounding verrucous lesions.1 There is a unique report of infection of an epidermal cyst by E. histolytica, in the absence of concomitant intestinal disease.16
Differential diagnosis A diagnosis of CL may easily be overlooked by histopathologists who are seldom exposed to biopsy material from such cases, especially when not alerted to a significant travel history. This is particularly the case when organisms are sparse or if unusual histologic features are present, such as sarcoidal granulomas, tuberculoid granulomas, palisaded granulomas with central fibrinoid change, elastophagocytosis, and conspicuous numbers of multinucleated histiocytic giant cells. Lesions may thus be misdiagnosed as sarcoidosis, foreign body granuloma, granuloma annulare, or lupoid rosacea.61–63
Histologic features The trophozoites of E. histolytica are found among the purulent exudate of the ulcer and are seen more clearly with PAS staining (Fig. 18.253). They are 12–20 µm in diameter and are distinguished by their tendency to phagocytose red cells; the presence of these hematophagous amebic trophozoites is diagnostic, and is regarded as an unequivocal sign of their pathogenicity. Lesions may be superficial or deep, with the latter involving the subcutis. Necrosis is common and may be liquefactive, coagulative, or suppurative.1–3 Trophozoites and cysts are usually found in the patient’s
921 Infections caused by free-living amebae
A
B
acanthamebiasis and balamuthiasis have received increasing recognition as opportunistic pathogens in immunocompromised patients, especially debilitated, malnourished hosts and those with HIV/AIDS.1–14 Acanthamoeba spp. appears to be more important in immunosuppressed organ transplant recipients and those with GVHD.15–19 Transmission of B. mandrillaris via organ transplantation has been reported.20 Infection with B. mandrillaris (formerly referred to as leptomyxid ameba) may nevertheless occur in immunocompetent individuals, including children.1–3,21,22
Acanthamebiasis is a condition reported almost exclusively from the United States, although cases have occurred in Korea and South Africa (personal observation).2,3,23 Although the majority of B. mandrillaris infections reported in the past were from the United States, balamuthiasis is an emerging infectious disease in parts of South America, especially in Peru.1–4,12,20,24 There have also been rare reports of the latter condition from Thailand, India, and Australia.14,21,22,25–31
feces. The organisms are surrounded by neutrophils, with some lymphocytes and plasma cells. The adjacent epidermis appears acanthotic and this may be marked or pseudoepitheliomatous in verrucous forms. Spongiosis may be conspicuous in superficial lesions.1
Differential diagnosis E. histolytica infection is distinguished from infection with free-living amebae (Acanthamoeba spp. and B. mandrillaris) by the presence of erythrophagocytosis in the former condition. The diagnosis may nevertheless be confirmed with the aid of newer molecular techniques.7
Infection with Acathamoeba spp. or B. mandrillaris results in an often fatal progressive encephalitis, and associated cutaneous lesions are a frequent occurrence.1–5,7,12 Visceral dissemination to organs such as the lungs, kidneys, and uterus may also occur.1,17 Spread of Acanthamoeba spp. to the CNS and skin is usually from a primary source of infection in the lungs or paranasal sinuses.2,6,23 Involvement of the skin may be the presenting manifestation of disseminated infection.5 Isolated cutaneous disease with chronic, nonhealing ulcerated skin lesions may be the sole manifestation in patients with AIDS-associated acanthamebiasis (Fig. 18.254).8 Acanthamebiasis of the skin presents as multiple deep dermal and subcutaneous nodules, usually on the extremities and face.5,7,13,15,16,19 Necrotizing panniculitis may occur.9 Pustular, ulcerating, purpuric, and sporotrichoid lesions have also been described.6,7,32
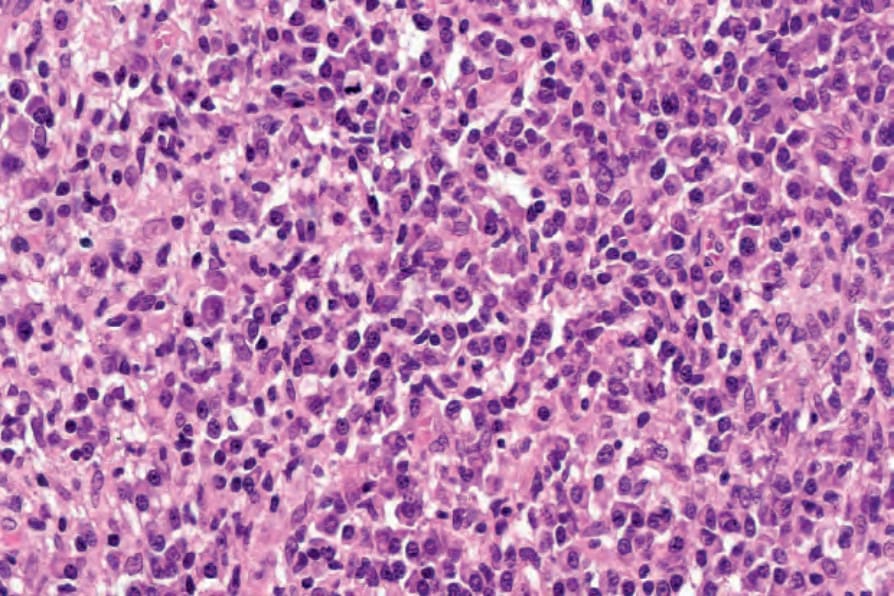
Fig. 18.251 Post-kala-azar dermal leishmaniasis: in this example, organisms are no longer visible.
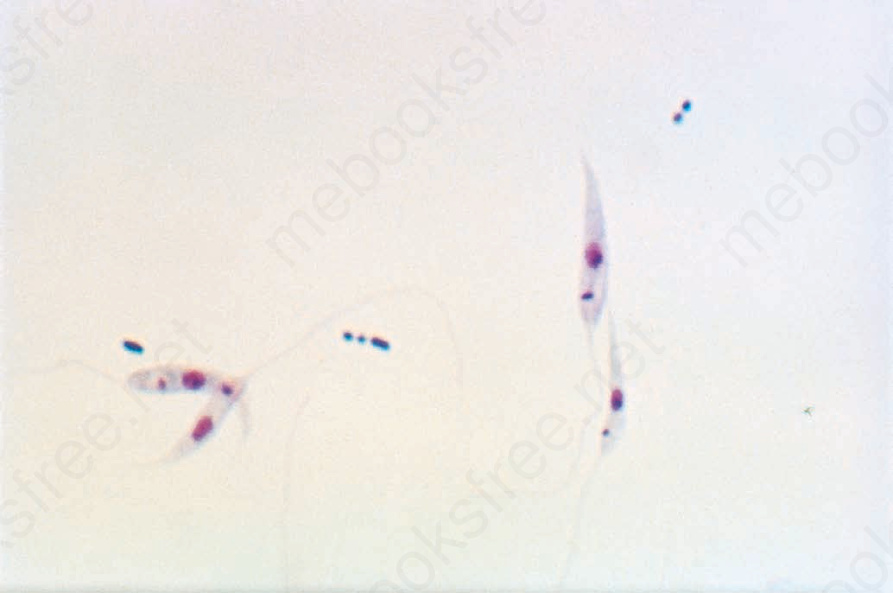
Fig. 18.252 Visceral leishmaniasis: promastigote forms of Leishmania donovani; note the anterior kinetoplast and flagellum (the latter is not seen in human infection) (Giemsa stain). By courtesy of H.P. Lambert, MD, and the London School of Hygiene and Tropical Medicine, London, UK.
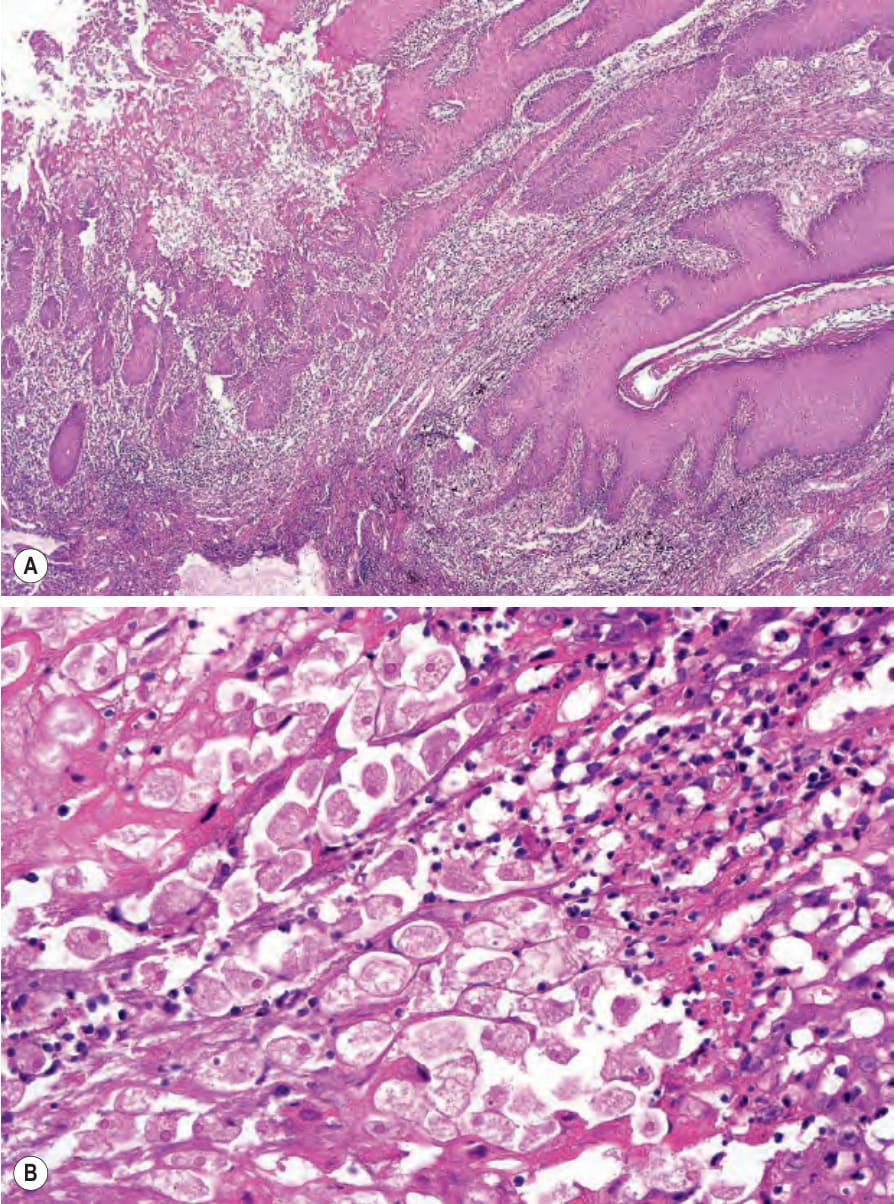
Fig. 18.253 Amebiasis cutis: (A) this biopsy is from a woman with vulval ulceration due to direct spread from the anus; the epithelium is hyperplastic and the lamina propria is chronically inflamed. (B) There are numerous trophozoites present; note the ingested red cells.

Fig. 18.254 Acanthamebiasis: there are widespread ulcers in this HIV-positive patient. There was underlying vasculitis. Courtesy of N.-N. Moti-Joosub, MD, Division of Dermatology, University of the Witwatersrand, Johannesburg, South Africa.