Leishmaniasis
Leishmaniasis
the years these investigations have been complemented or superseded by serology, culture, or more recently, PCR-based methods.5,9,19–21
Clinical features Leishmania is a protozoan parasitic organism related to the trypanosomes. The life cycle contains a flagellate phase (promastigote) which occurs in the intestine of its vector, a female Phlebotomus or Lutzomyia sandfly, and a phase in which the flagellum is retracted (amastigote). The latter is the form seen in the human host. Various mammals, including gerbils, rodents, dogs, jackals, hyraxes, and foxes, may act as reservoirs of infection.1–7
An estimated 12 million people are affected worldwide in 102 countries, areas, and territories, and on 5 continents. As many as 1.2 million new cases occur annually, the majority of whom have cutaneous leishmaniasis (CL), while some 400 000 develop visceral leishmaniasis (VL).7–10 After malaria, leishmaniasis is the second leading cause of protozoal-related deaths worldwide, with an estimated 20 000 to 30 000 deaths annually.6 VL and, to a lesser extent, CL are increasingly recognized as opportunistic diseases in immunocompromised patients, especially those infected with HIV.8,11–15 Leishmaniasis may also be a manifestation of IRIS in HIV/AIDS patients on ART.7 Cutaneous involvement as a first indicator of underlying VL has been reported as a complication of anti-TNF-α therapy.16
Cutaneous leishmaniasis CL has many local names, including Oriental sore, Baghdad boil, Chiclero ulcer, and Aleppo boil. It is caused by L. tropica, L. major, and L. aethiopica and affects men, women, and children. Mediterranean CL is caused predominantly by L. infantum.17
Lesions occur on any site accessible to biting by the sandfly vector, most commonly the hands, arms, and face (Fig. 18.242). They present as an erythematous papule that enlarges over the course of a few weeks into an ulcerated and crusted nodule. Occasionally, multiple lesions are seen. Lesions show a tendency to orientation along the skin creases, and grossly the ulcers have been compared to a volcano in surface appearance and configuration.6,7,22 Variants may be hypoesthetic, psoriasiform, eczematous, varicelliform, paronychial, chancriform, zosteriform, annular, whitlow-like, erysipeloid, verrucous, or keloidal, or present as macrocheilia.17,23,24 Regional lymphadenopathy can be a feature.25
More than 20 species of Leishmania are responsible for human disease, and these are distinguished on the grounds of biochemical, antigenic, and genetic differences.6 Although leishmaniasis tends to be seen in Asia, Africa, the Americas, and the Mediterranean countries, it is being seen more often in nonendemic countries, particularly among refugees and returning holidaymakers.17,18 There are eight main types of cutaneous presentation, with many local geographic and species variations.
In endemic regions, a significant number of people appear to have asymptomatic (subclinical) infection, so-called cryptic leishmaniasis.17
Confirmation of the diagnosis has traditionally been achieved by visualization of the organisms in smears or tissue sections, or with the aid of the Montenegro (leishmanin) skin test, especially in the developing world. Over
In the Eastern hemisphere, where the disease has traditionally been referred to as, ‘Old World’ leishmaniasis, these lesions may be ‘wet’ or ‘dry’:
• The wet type has a short incubation period (2 weeks) and occurs in rural areas. It is caused by L. major and develops like a suppurative folliculitis which ulcerates, the surrounding edematous, indurated erythema extending gradually to reach a maximum of 6 cm. Small secondary nodules may be seen around this. Slow resolution with cribriform scarring occurs over 3–12 months.
• The dry form is caused by L. tropica, has a longer incubation period (2 months), and is mostly seen in urban areas.26 The initial lesion is a brown nodule and this becomes a plaque up to 2 cm across. It may ulcerate centrally with a firm crust. Resolution occurs with scarring over 12 months or longer. L. killicki is a recently identified subpopulation of L. tropica, and occurs in North Africa.27
917 Leishmaniasis
A
B
presentation is typically encountered in Eastern hemisphere leishmaniasis, a small number of cases of leishmaniasis recidiva cutis complicating American leishmaniasis have been reported.32–34
Skin infections with L. (V.) braziliensis are liable to recur as mucosal lesions, known as espundia (in which there is much tissue destruction), sometimes years later. The mucosal lesions occur most often in the nasal septum and mouth and rarely around the eyes, genitalia, and anus (Fig. 18.244). Patients may also develop ‘tapir nose’ in which there is considerable damage to the nasal cartilage resulting in a free-hanging nose.17 The mucosal lesions start as superficial erosions, but become deeply ulcerative and destructive. The Montenegro skin test is almost always positive.
The American forms, traditionally referred to as ‘New World’ leishmaniasis, are caused predominantly by L. mexicana and L. (subgenus Viannia) braziliensis. Other species implicated include L. amazonensis, L. (V.) guyanensis, L. (V.) panamensis, and L. (V.) peruviana.28,29 The lesions of L. mexicana are usually like those of CL in the Eastern hemisphere, but some subvariants can cause destructive ulceration of the ear. Most infections with L. (V.) braziliensis are local and heal without much damage.
Diffuse CL, also known as pseudolepromatous leishmaniasis, is caused by variants of L mexicana and L. aethiopica. The former occurs in Bolivia, Venezuela, Mexico, and Brazil, while the latter is seen predominantly in Ethiopia. It develops as a consequence of an impaired cellular immune response.31 A study from Egypt showed a significant association between histocompatibility antigens HLA-A11, B5, and B7 and the occurrence of this disease.35 It begins as a nodule, which grows and becomes surrounded by other similar lesions. This process is repeated until eventually, over many years, most of the skin becomes nodular (Fig. 18.245). The nodules do not ulcerate and can closely resemble LL. Although lesions may develop in the nasal mucosa, these are not destructive like those of the mucocutaneous form of American leishmaniasis. Response to therapy is slow and relapse is common. The Montenegro test is invariably negative.
Chronic CL represents persistence (or spread) of an acute lesion for more than 1 year. Lesions are particularly seen on the face as raised erythematous plaques which may resemble erysipelas (Fig. 18.243).17 The erysipeloid lesions are erythematous and infiltrative and are said to occur more frequently in women older than 50 years.30
The acute lesions may be followed by a relapsing chronic or lupoid stage (leishmaniasis recidivans or leishmaniasis recidiva cutis) in which brownish papules develop close to the scar of the earlier stages. This occurs in 3% to 10% of patients.31 These papules extend to resemble lupus vulgaris; they may develop hypertrophic scars or become verrucous. They are extremely slow to resolve, even under treatment, and may persist for many years. It is thought that a change in local immunity results in reactivation of intracytoplasmic organisms.31 The leishmanin or Montenegro skin test for cellular immunity to Leishmania is strongly positive in nearly all cases. It has been suggested that leishmaniasis recidivans represents a hypergic form of the disease, but this has been disputed by others.32 Although this
L. major and L. (V.) panamensis may be associated with a sporotrichoid spreading reaction.8
There have been rare reports of neoplasms such as basal cell carcinoma, squamous cell carcinoma, or even dermatofibrosarcoma protuberans arising in scars associated with CL.7,36–39
Visceral leishmaniasis VL (kala-azar, black fever) is due to infection by L. donovani complex and occurs widely in South America (L. chagasi), Africa (L. infantum), the Mediterranean (L. infantum), and Asia (L. donovani and L. infantum).9,40,41 It may be a manifestation of HIV infection.8,11,42 In patients with HIV/AIDS,
918 Infectious diseases of the skin
A
Pathogenesis and histologic features In all variants of the disease, the amastigote form of the parasite multiplies within the histiocytes of the mammalian host. The host response is related to the number of amastigotes and the degree of cellular immunity. Large numbers of amastigotes are associated with an anergic response and many histiocytes without other inflammatory cells. Moderate numbers of amastigotes are usually associated with necrosis, which is an important mechanism for eliminating infection. Smaller numbers are associated with a good epithelioid granulomatous response after the necrosis phase. Some infections are eliminated by an effective granulomatous response without necrosis, while others are associated with focal necrosis and ulceration when organisms are released. In others, there is more extensive necrosis. The events following necrosis depend on the rate at which an effective epithelioid granulomatous reaction develops.50,51 An unusual case of late-stage CL harboring foci of caseous necrosis with no demonstrable organisms has been reported.52 Healing is often relatively rapid once necrosis has occurred. In parallel with developing immunity, the overlying epidermis shows pseudoepitheliomatous hyperplasia. Lymphocytes and plasma cells also become more numerous at the periphery of the granuloma. Scarring eventually replaces the granuloma.
B
leishmaniasis may occur in herpes zoster lesions, and dermatofibroma cells may be parasitized by the organisms. Nodular cutaneous lesions arising in AIDS-related VL may mimic Kaposi sarcoma clinically.43 Following inoculation, the organisms multiply in histiocytes; the onset of disease is insidious, taking 2–4 months. The macrophages of the liver and spleen take up the organisms, resulting in hepatosplenomegaly associated with lymphadenopathy, pancytopenia, irregular and intermittent fever, and marked weight loss. In India, some patients develop earthy-gray pigmentation, particularly on the temples, around the mouth, and on the hands and feet.17
A small number of patients who recover subsequently develop post-kalaazar dermal leishmaniasis (PKDL).44–46 This has been reported from India and East Africa. The lesions start as erythematous or hypopigmented macules (particularly on the face) and become nodular and coalesce so that they closely resemble LL, but they lack sensation abnormalities. The lesions are persistent, but resolve slowly on treatment.46–48 Co-infection with VL and leprosy has been reported from countries where both conditions are endemic, including leprosy and PKDL.49
The recent identification of Leishmania RNA virus (LRV)-1 and LRV-2 in New World and Old World Leishmania spp. is of particular interest. Recognition of the replicated virus by the host’s TLR3 initiates destruction of the parasite, with dispersal of LRV and the subsequent release of proinflammatory chemokines and cytokines.7,53

Fig. 18.242 Cutaneous leishmaniasis: (A) this healing lesion shows crusting and scarring; (B) there is an extensive ulcerated erythematous plaque with scaling. (A) By courtesy of J.C. Pascual, MD, Alicante-Spain; (B) from the collection of the late NP Smith MD, the Institute of Dermatology, London, UK.
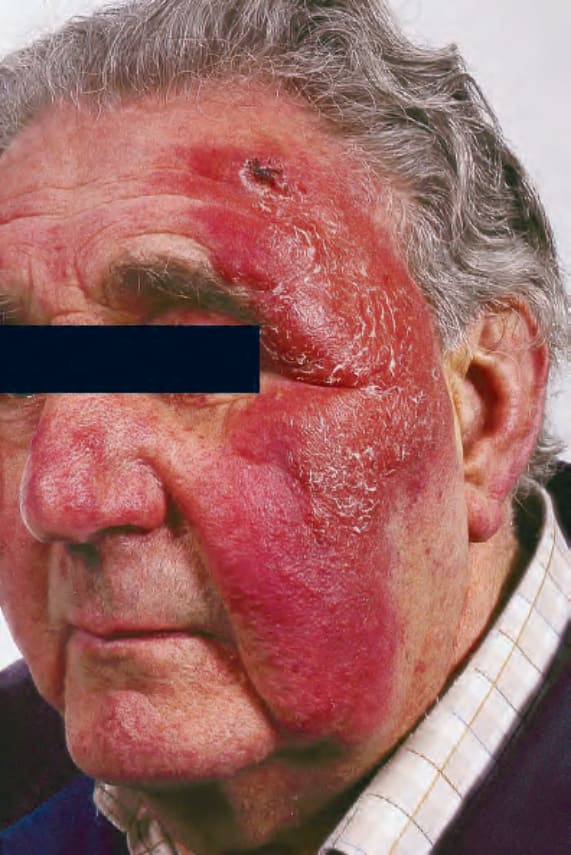
Fig. 18.243 Cutaneous leishmaniasis: chronic cutaneous leishmaniasis showing intense edema, erythema, and scaling. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.

Fig. 18.244 (A, B) Mucocutaneous leishmaniasis: the lesions are destructive and very disfiguring. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.

Fig. 18.245 Diffuse cutaneous leishmaniasis: note the widespread lesions, many of which appear keloidal. By courtesy of the late M.S.R. Hutt, MD, St Thomas’ Hospital, London, UK.
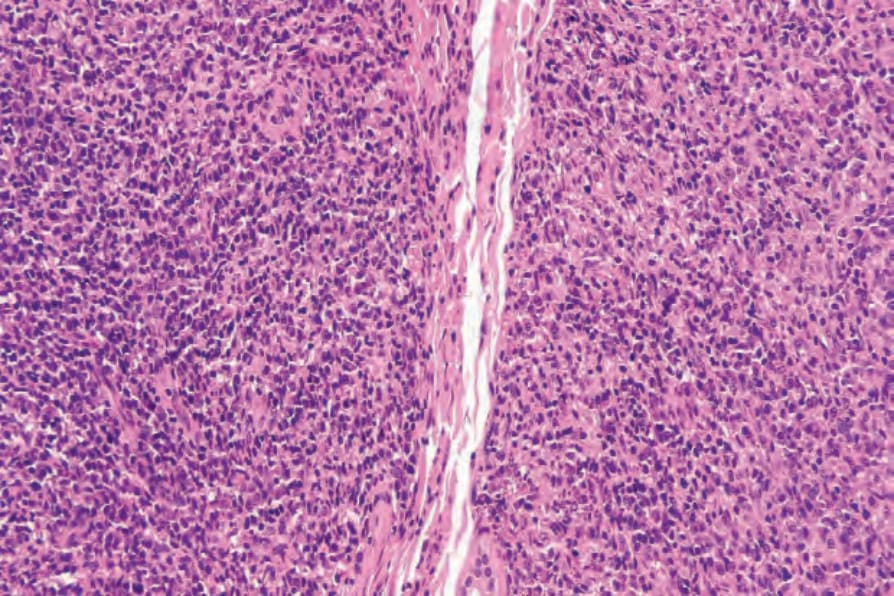
Fig. 18.250 Post-kala-azar dermal leishmaniasis: there is a heavy mixed infiltrate of histiocytes, lymphocytes, and plasma cells.
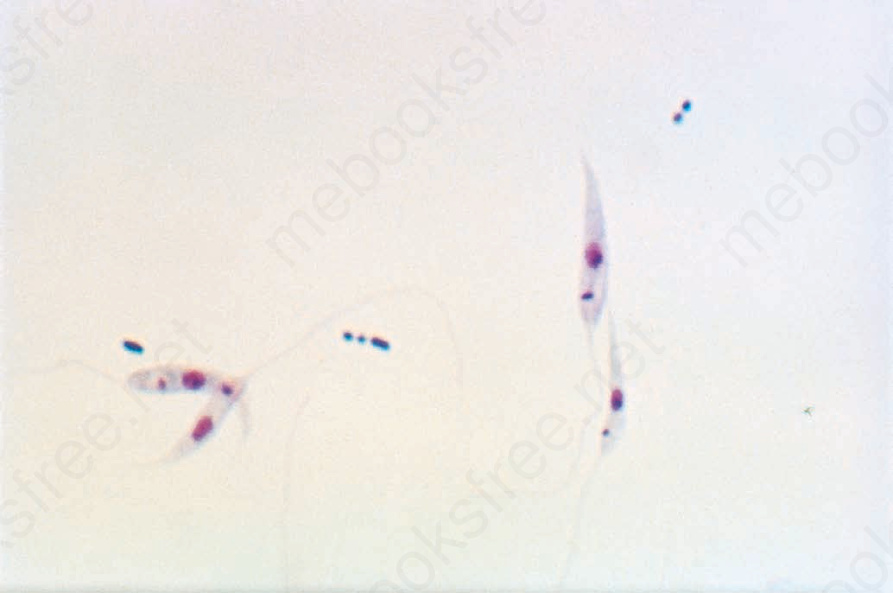
Fig. 18.252 Visceral leishmaniasis: promastigote forms of Leishmania donovani; note the anterior kinetoplast and flagellum (the latter is not seen in human infection) (Giemsa stain). By courtesy of H.P. Lambert, MD, and the London School of Hygiene and Tropical Medicine, London, UK.
Histologically, the acute lesion (oriental sore) is characterized by hyperkeratosis and acanthosis, although occasionally epidermal atrophy and parakeratosis are features.31 Ulceration is frequently seen (Fig. 18.246). Liquefactive degeneration of the basal keratinocytes has been described.31 The epidermis may show pseudoepitheliomatous hyperplasia, and intraepidermal neutrophil microabscesses are not infrequent. The dermis typically contains an intense infiltrate of histiocytes, lymphocytes, and plasma cells. Rarely, a Grenz zone is evident. Neutrophils and eosinophils are usually sparse.54 Large numbers of amastigotes are evident and these may be seen within the overlying keratinocytes (Fig. 18.247).31,54 Foci of dermal necrosis may be evident. Vascular changes are usually not seen.54 Perineural and
919 Leishmaniasis
intraneural chronic inflammatory changes associated with perineural Leishmania organisms have been described.55 The patient was found to be hyperesthetic clinically. In chronic lesions, the dermis contains large numbers of small noncaseating granulomata (Fig. 18.248). Giant cells tend to be sparse. Leishman bodies are sparse or absent.31 Necrosis is very rare at this stage.54
Histologically, mucocutaneous leishmaniasis is extensively necrotic, with many plasma cells, lymphocytes, neutrophils, and macrophages, but few organisms. Occasional tuberculoid or suppurative granulomata may be present.1,3
As with LL, diffuse CL is characterized histologically by numerous macrophages distended with amastigotes and a lack of granuloma formation. There are few lymphocytes and plasma cells. These features indicate anergy, but not primary immunodeficiency.
The features of PKDL are similar to those of the diffuse cutaneous variety; the overlying epidermis is atrophic, but is not usually ulcerated (Figs 18.249–18.251). Nodular lesions show a dense dermal lymphohistiocytic infiltrate. There are a variable number of organisms. Vascular hyalinization is evident, and marked follicular plugging may be observed.56 Degeneration
of basal epidermal keratinocytes was observed in one study. The dermal infiltrate was noted to comprise T-lymphocytes and macrophages, with a preponderance of CD4+ T-cells over CD8+ lymphocytes. Plasma cells, however, were inconspicuous or absent.57
The lupoid form of chronic CL may be difficult to diagnose because it represents an exaggerated tuberculoid response to very few organisms (and as such, closely resembles lupus vulgaris) or perhaps only leishmanial antigen; it is best distinguished from other tuberculoid diseases on the basis of its positive Montenegro skin test.31 There is no necrosis, and plasma cells are sparse.
In all other forms of CL the diagnosis is confirmed by the demonstration of amastigotes in a smear or skin section.58 The organisms are best revealed by Giemsa stain as reddish cytoplasmic round to oval structures
920 Infectious diseases of the skin
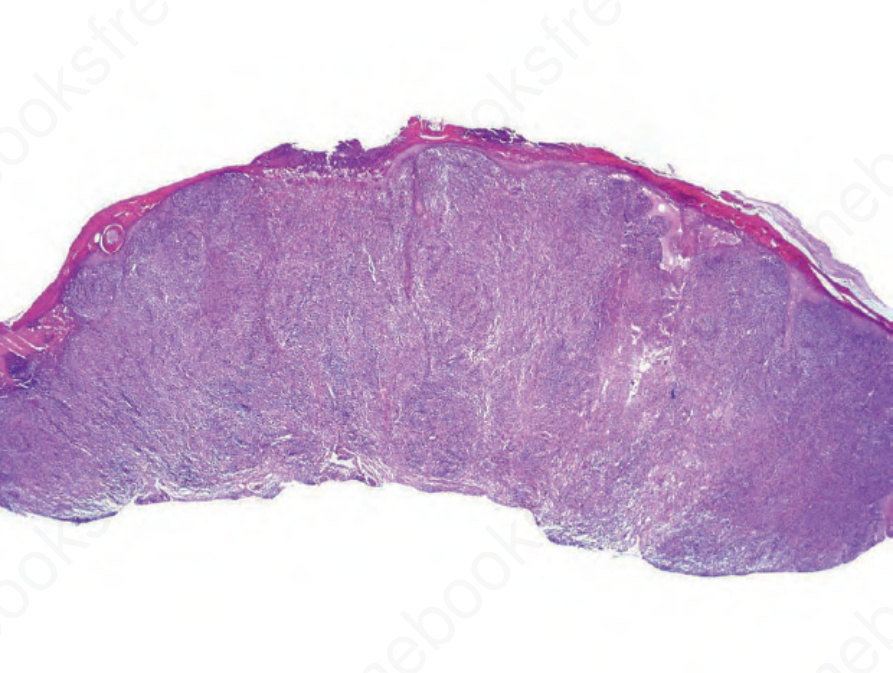
Fig. 18.246 Oriental sore: there is extensive ulceration and the adjacent epithelium is acanthotic; intense inflammation is seen deep to the ulcer bed.
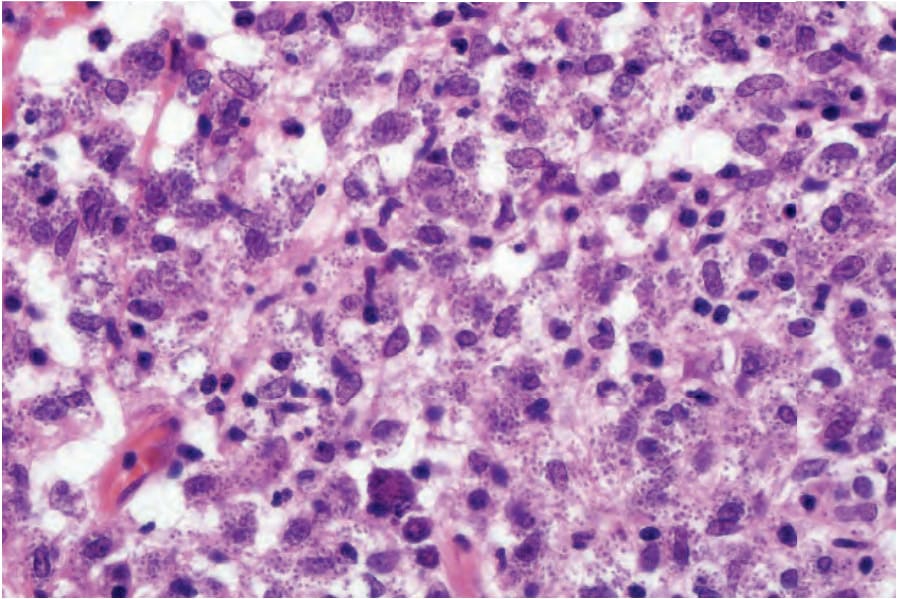
Fig. 18.247 Oriental sore: the infiltrate consists of parasite-laden histiocytes with small numbers of lymphocytes.
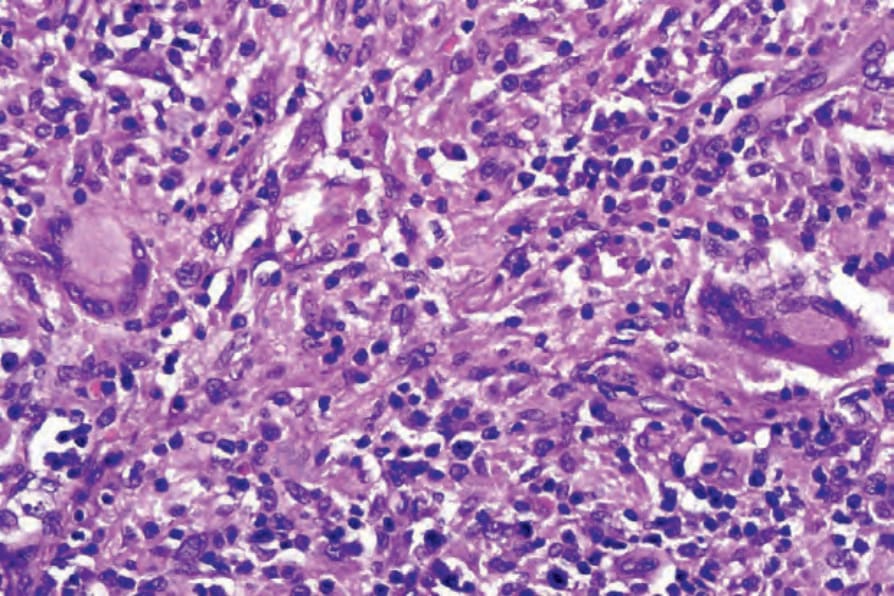
Fig. 18.248 Oriental sore: epithelioid cell granulomata as seen in this field are a feature of chronic lesions.
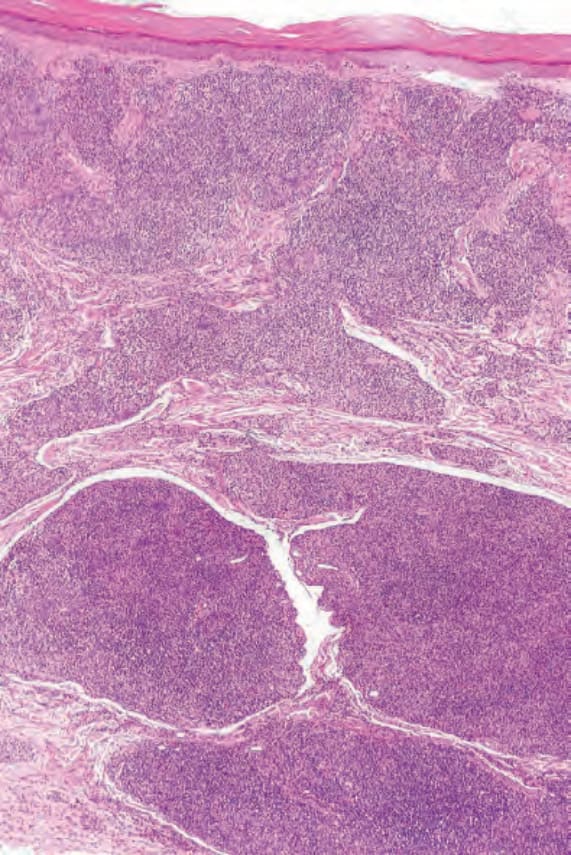
Fig. 18.249 Post-kala-azar dermal leishmaniasis: there is a dense dermal nodular infiltrate. The Grenz zone is spared.