Malakoplakia
Malakoplakia
Clinical features Malakoplakia (soft plaque) most often affects the urinary tract, but it can involve many other organs including the gastrointestinal tract, lymph nodes, genitalia, brain, bone, lungs, retroperitoneum, adrenals, tongue, and skin.1–7 The median age at presentation is approximately 53 years, and the disease appears to be twice as common in males as in females.4 Cutaneous lesions are most common around the genitalia or perineum, but are occasionally seen in other sites.3–8 Their appearance is variable and includes plaques, ulceration, polyps, and sinuses, with surrounding induration, as well as nodules and papules.5,7,9 They may be associated with malakoplakia elsewhere.
B
Underlying or associated conditions (which are usually linked with immunosuppression) can include carcinoma, rheumatoid arthritis, SLE, diabetes mellitus, leukemia, lymphoma, and immunosuppression following transplantation.3,4,10–12 However, the condition remains distinctly uncommon in patients with HIV/AIDS; this has been ascribed to selective or relative preservation of antimicrobial monocytic function.9,13 The skin lesions are nonprogressive but are persistent.
Pathogenesis and histologic features Although the exact pathogenesis of malakoplakia is poorly understood, the condition is thought to be secondary to an acquired bactericidal defect occurring within macrophages.6,12 Lesions of malakoplakia are characterized by confluent sheets of histiocytes (von Hansemann cells) with eosinophilic granular cytoplasm and small, usually eccentric nuclei. These cells also contain characteristic cytoplasmic basophilic bodies shown to be calcified with von Kossa staining (Figs 18.226 and 18.227). These round, sometimes laminated structures are known as Michaelis-Gutmann bodies. Their targetoid pattern is accentuated by staining with PAS. They may also be positive on staining with Perl reaction for iron. The Michaelis-Gutmann body is sufficiently distinctive to allow cytological distinction of malakoplakia in a preparation from skin scrapings.14 Immunohistochemistry with an antibody to BCG may highlight the intracytoplasmic bacteria.15
The abscess persists with numerous sinuses and extensive fibrosis, and may extend to involve deep adjacent structures. Rarely, the granules are eliminated transepithelially.21 The reasons for the persistence and for granule formation are not fully understood. Although some patients show immunodeficiency, sometimes analogous to the anergy of LL, this is not so for most cases. The size of the original inoculum appears to be critical – excessive numbers of bacteria produce an overwhelming abscess and cellulitis, too few bacteria are rapidly eliminated by normal inflammatory responses – but an intermediate size of inoculum can produce what may be interpreted as a balance between the bacteria and the inflammatory response, with granule and chronic abscess formation.1,2,22 This balance may be attained more easily with less virulent strains.
A foreign body may contribute to the initiation of the lesion, but is not invariable. A local factor may be important, such as some as yet undemonstrated defect in the cutaneous immune mechanisms, diabetes mellitus, or an underlying dermatosis such as follicular mucinosis.23,24 In pulmonary cases,
The histiocytic infiltrate may be mixed with neutrophils, lymphocytes, and plasma cells, with associated granulation tissue. Electron microscopy of malakoplakia shows that the histiocytes contain numerous phagolysosomes
909 Actinomycosis
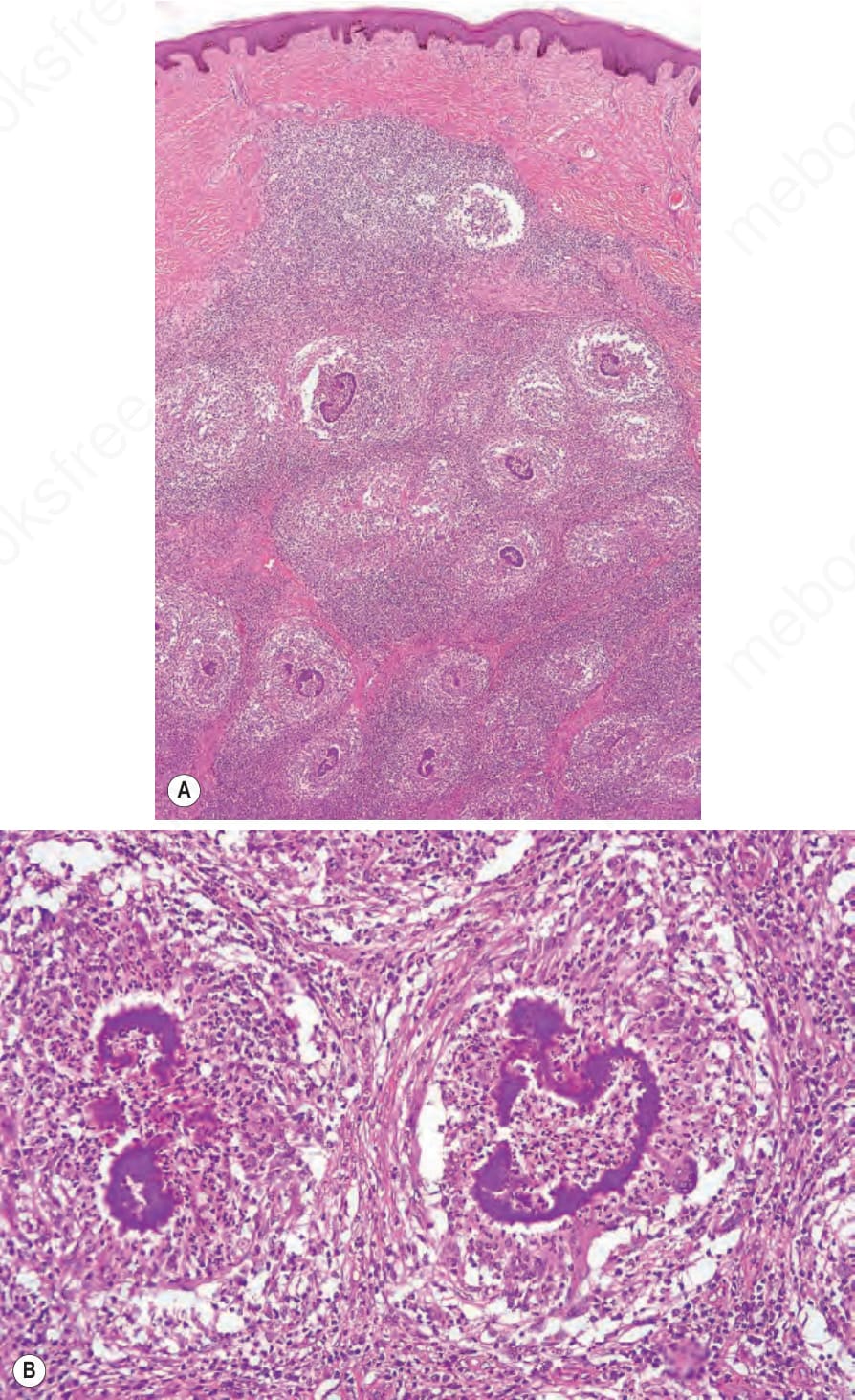
Fig. 18.224 (A, B) Botryomycosis: there are multiple dermal abscesses surrounding discrete bacterial colonies.
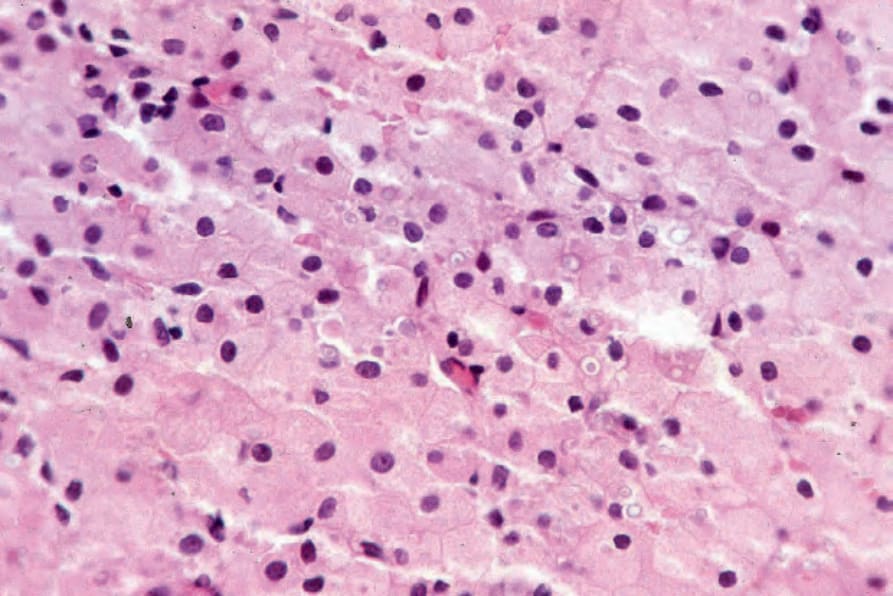
Fig. 18.226 Malakoplakia: the infiltrate consists of histiocytes with eosinophilic granular cytoplasm. Note the pale blue, laminated Michaelis-Gutmann bodies.

Fig. 18.228 Actinomycosis: extensive intrathoracic disease has resulted in involvement of the anterior chest wall. Numerous sinuses are evident. By courtesy of P. Duhra, MD, Coventry and Warwickshire Hospital, Coventry, UK.