Botryomycosis
Botryomycosis
Clinical features Botryomycosis (Gr. botrys, bunch of grapes) is also known as bacterial pseudomycosis and is due to a chronic bacterial infection, usually of skin.1–3 It has also been described in lung, bone, kidney, and liver.1–7 A case of gingival botryomycosis resembling a lobular capillary hemangioma (pyogenic granuloma) has been reported.8
In the skin, the lesions are chronic suppurative nodules which may resemble infected epidermoid cysts, plaques, and ulcers. The interconnecting fistulae which develop give it a similarity to acne conglobata and hidradenitis suppurativa, but the sites commonly involved are the hands, feet, and head.1,9 There may be a history of preceding trauma or the presence of a foreign body.9,10 Deeper tissues, including muscle and bone, may become involved. Botryomycosis of the cervicofacial region has also been described in a patient with mandibular chronic osteomyelitis.4
B
The pulmonary involvement has the radiological features of lobar consolidation, sometimes with adjacent osteomyelitis. Involvement of liver, tongue, orbit, bowel, and brain has also been described. Cystic fibrosis appears to predispose to some pulmonary cases. Although immunodeficiency has been noted in some cases and the condition has been reported in association with HIV/AIDS, most patients who develop botryomycosis have no detectable abnormality of the immune system.11–16 The cutaneous lesions of botryomycosis in patients with HIV/AIDS may, however, present with atypical features; lesions resembling prurigo nodularis, lichen simplex chronicus, and pruritic papules have been described.14,16 Disseminated botryomycosis is very rare.17
a feature of greater virulence or less immunity; methenamine silver is most satisfactory for demonstrating the filaments in tissue sections.
The histologic features in the skin are of ulcers, abscesses with pus, necrosis, hemorrhage, and fibrosis associated with sinus tracks. The organism is not readily seen with H&E staining, but can be demonstrated histologically by its weak acid-fastness, distinguishing it from Actinomyces. Differential culture may be necessary to distinguish the two, although the presence of sulfur grains is a pointer toward actinomycosis.49
Pathogenesis and histologic features The lesions of botryomycosis include a characteristic granule surrounded by suppuration and the features of a chronic abscess. The granule consists of nonfilamentous bacteria in a hyaline matrix, containing IgG and complement C3 (the Splendore-Hoeppli phenomenon), and is a lobulated or ‘bunch of grapes-like’ structure (Figs 18.224 and 18.225).13,18 The granule is basophilic in the center and eosinophilic at the periphery.1 It is PAS positive. The bacteria present are not specific to the condition; S. aureus is most common, but Pseudomonas, E. coli, Proteus, Micrococcus, and streptococci may also be found.1,4,14,19 Fungi, actinomycetes, and Nocardia are not causes. There have, however, been isolated case reports of botryomycosis due to combined S. aureus and Actinobacillus actimomycetemcomitans infection, and S. aureus in association with Pneumocystis jiroveci.15,20
908 Infectious diseases of the skin
A
cystic fibrosis represents that local underlying defect. Botryomycosis with concurrent cutaneous small vessel vasculitis has been documented.25

Fig. 18.222 Nocardiosis: (A) this cutaneous nodule developed in an immunocompromised young male; (B) a different lesion is shown in close-up. By courtesy of R.A. Marsden, St George’s Hospital, London, UK.
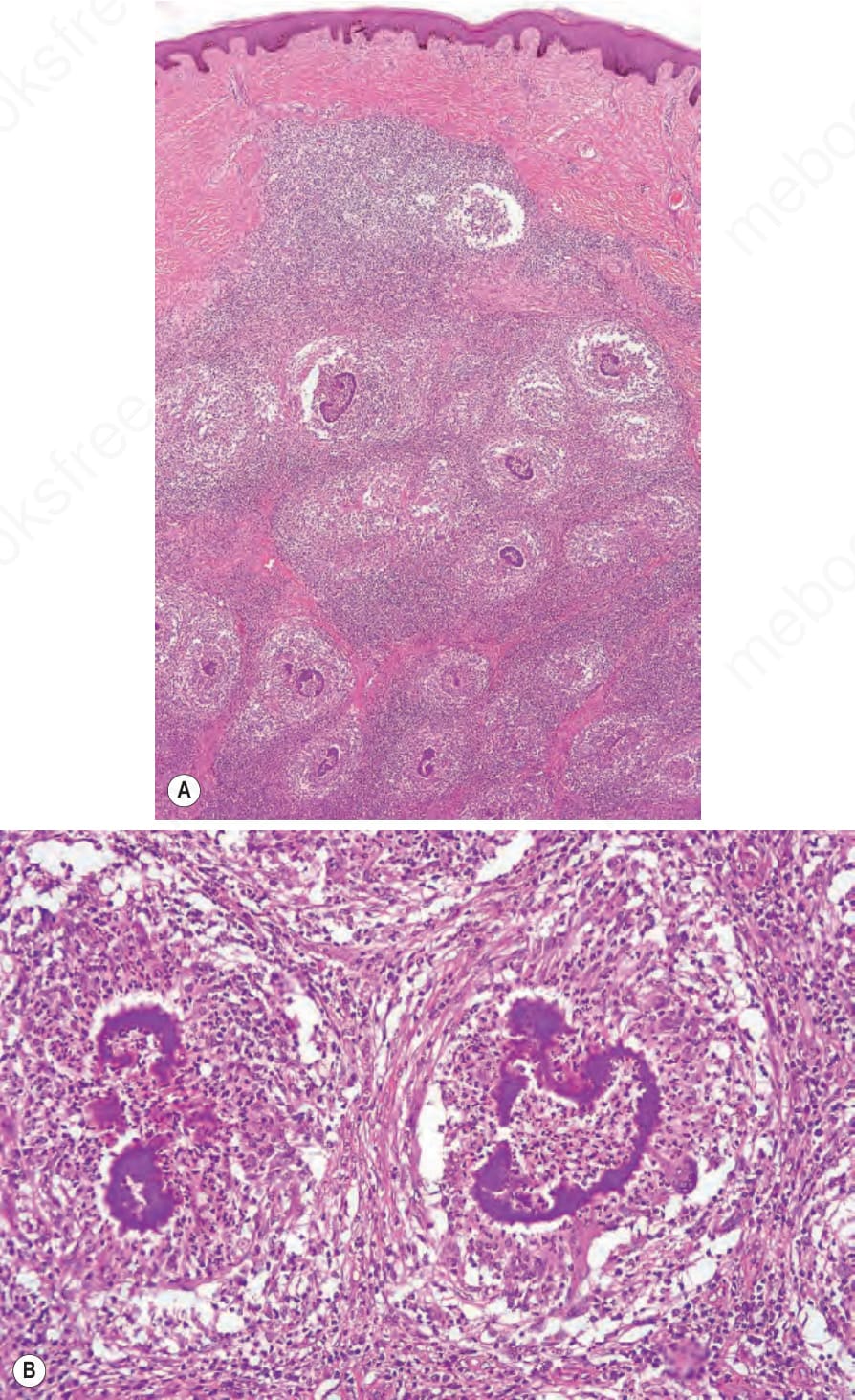
Fig. 18.224 (A, B) Botryomycosis: there are multiple dermal abscesses surrounding discrete bacterial colonies.
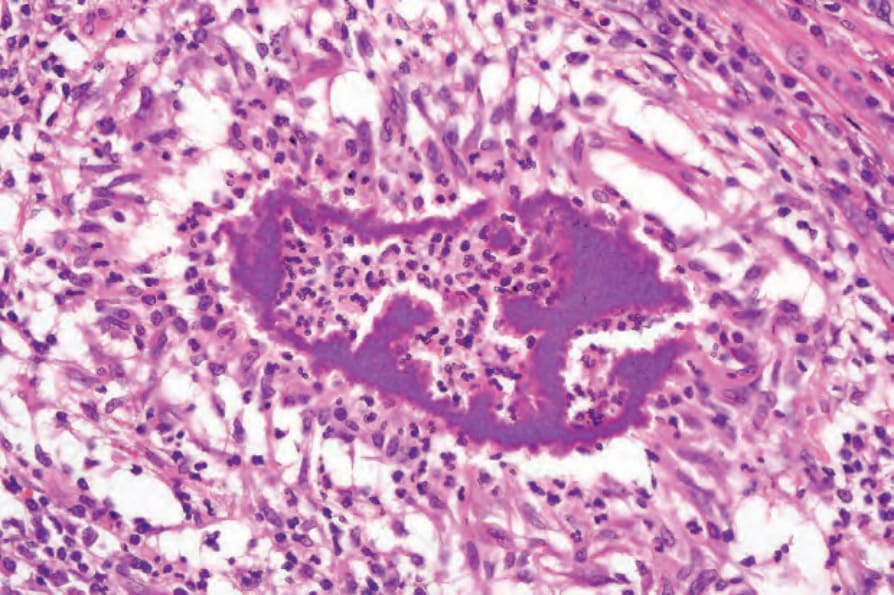
Fig. 18.225 Botryomycosis: note the blue-staining bacteria surrounded by an intensely eosinophilic fibrillary coat (the Splendore-Hoeppli phenomenon). The inflammatory response is characteristically neutrophil mediated.