Rhinoscleroma
Rhinoscleroma
Clinical features Rhinoscleroma is usually seen in young adults and is now largely confined to the tropics and subtropical regions; it was, however, previously common in Eastern Europe.1–4, The disease has been linked to poor socioeconomic conditions and is still encountered in parts of Central Africa, Southeast Asia, India, Mexico, as well as Central and South America.4–6 Rhinoscleroma has also been described in the Arabian Gulf, and is considered endemic in Egypt.1,6,7 It is a severe chronic infection of the upper respiratory tract, especially the nose. The disease is contracted via direct droplet infection or, more indirectly, by contamination of material that is subsequently inhaled. It has a very long incubation period.
There are three phases to the clinical features of the disease:
• It begins with a catarrhal phase, with symptoms suggesting a non-specific rhinitis or coryza with frontal headaches.3 These symptoms persist for weeks or months, becoming gradually more severe with superimposed epistaxes and difficulty in nasal breathing associated with swollen mucous membranes.3,8
• An infiltrative phase follows during which the nasal septum and base of the nasal fossa become swollen by a reddish waxy induration.3 This change is painless and the soft palate is anesthetic. Similar involvement of the larynx causes changes in the voice.
• The infiltrative phase merges into a nodular phase during which there is increasing deformity as the nose, upper lips, and gums become grossly enlarged and distorted.3,8 Involvement of regional lymph nodes is not usual, but has been reported.9 Nasal obstruction, loss of smell, loss of voice, laryngeal stenosis, and increasing difficulty with breathing may follow.5,8,10 Respiratory obstruction may cause death; alternatively, the process can persist with some temporary remissions for years. Squamous carcinoma is an occasional late complication. Contiguous involvement of the soft and hard palate, the upper lip, and the maxillary sinuses may occur; the term respiratory scleroma has been proposed for these cases with extranasal extension of the disease.11 Involvement
numbers of bacilli.46 Marked intraendothelial cell bacillary proliferation is characteristic.31,77 It has been suggested that this feature is indicative of a very poor immune response facilitating antigen-antibody interaction with consequent acute necrotizing vasculitis. This seems to be rather unlikely (on its own) as similar numbers of leprosy bacilli have been described in the endothelium of 100% of small vessels in untreated polar and subpolar LL.44,72
Histoid leprosy shows a spindle cell proliferative pattern suggestive of fibrous histiocytoma (Figs 18.214 and 18.215). A storiform pattern may be conspicuous. Careful examination, however, will reveal foci of Lepra cells. A Wade-Fite reaction reveals large numbers of bacilli, often arranged in sheaves.23,24
In type I (reversal) reactions, edema is observed both within and outside of the intradermal granulomas. Numerous histiocytic giant cells may also
904 Infectious diseases of the skin
A
A
B
B
of the nasolacrimal duct has also been described. A recurrence rate of up to 25% over a 10-year period was documented in an Egyptian series.1 Rosai-Dorfman disease has been documented in the regional lymph nodes of a patient with rhinoscleroma.12
Pathogenesis and histologic features The causative bacterium Klebsiella rhinoscleromatis is a Gram-negative aerobic diplobacillus.11,13 It is spread during the rhinitis (catarrhal) phase of the disease and appears to be confined to close-living groups, and has even been documented in siblings.14 There is no animal reservoir. An HLA- DQA103011-DQB10301 haplotype has been identified as a potential risk factor for development of the disease, while other investigators have suggested that altered lymphocyte subsets may play an important pathogenetic role.15,16
The incubation period is very long, so that presentation is most often in adults. The organism is phagocytosed, but not killed by neutrophils. When the neutrophils rupture, the still viable bacteria are phagocytosed by histiocytes, which become greatly distended. These eventually appear vacuolated
905 Nocardiosis
with an eccentric nucleus (Fig. 18.220). Warthin-Starry or Giemsa staining reveals that this vacuole contains bacteria (Fig. 18.221). This cell, 10–100 µm in diameter, is termed a Mikulicz cell and, together with Russell bodies (plasma cells grossly distended with proteinaceous product), is characteristic of the disease. As well as these characteristic cells, there is a dense infiltrate of plasma cells and lymphocytes, which becomes very extensive and eventually causes such gross thickening of the mucosae that the respiratory tract tends to be occluded at several points. The mucosa can be ulcerated or atrophic. Amyloid deposition has been described.6,17,18 The diagnosis may be confirmed by PCR.19 The occurrence of S100 immunoreactive histiocytes with emperipolesis in rare cases of rhinoscleroma has led some authors to speculate that the infection might play an etiological role in Rosai-Dorfman disease.20,21
Differential diagnosis This includes midfacial granulomata, lymphoma, tertiary syphilis, LL, leishmaniasis, and rhinosporidiosis. The histology, as described above, should exclude these clinical alternatives.
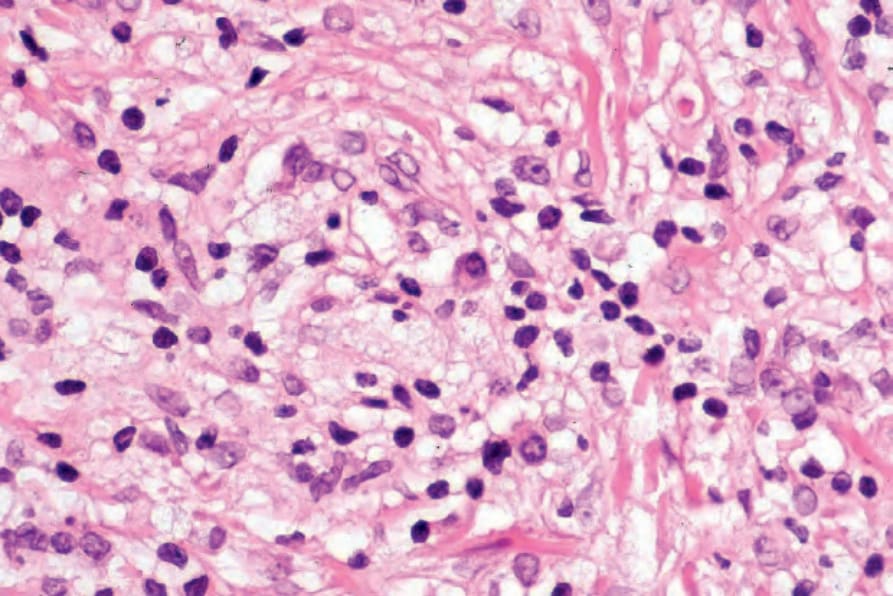
Fig. 18.210 Subpolar lepromatous leprosy: in addition to histiocytes and lymphocytes, there are conspicuous plasma cells.
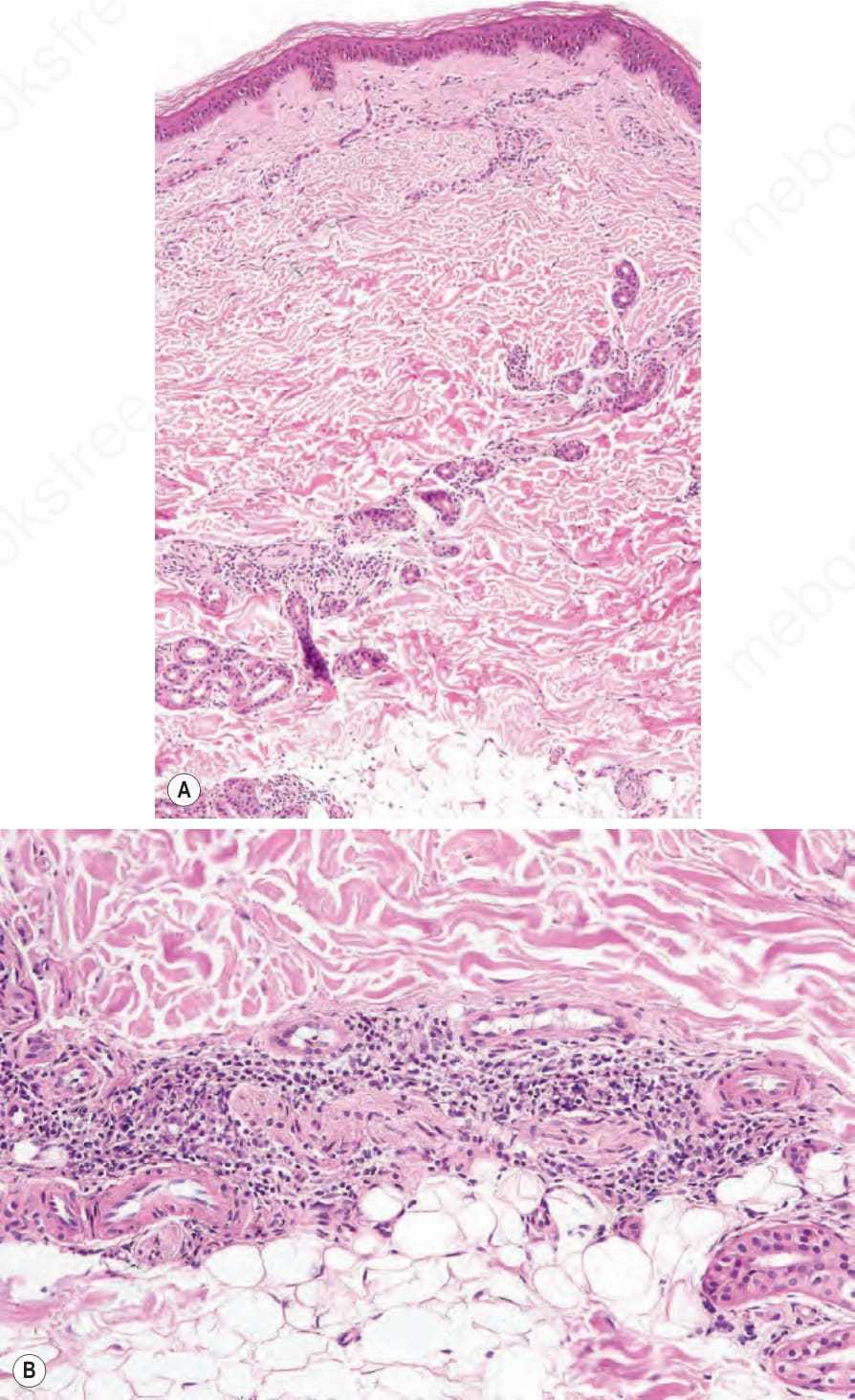
Fig. 18.212 (A, B) Indeterminate leprosy: a perivascular chronic inflammatory cell infiltrate is present in the deep dermis. Diagnosis depends on a high index of suspicion.
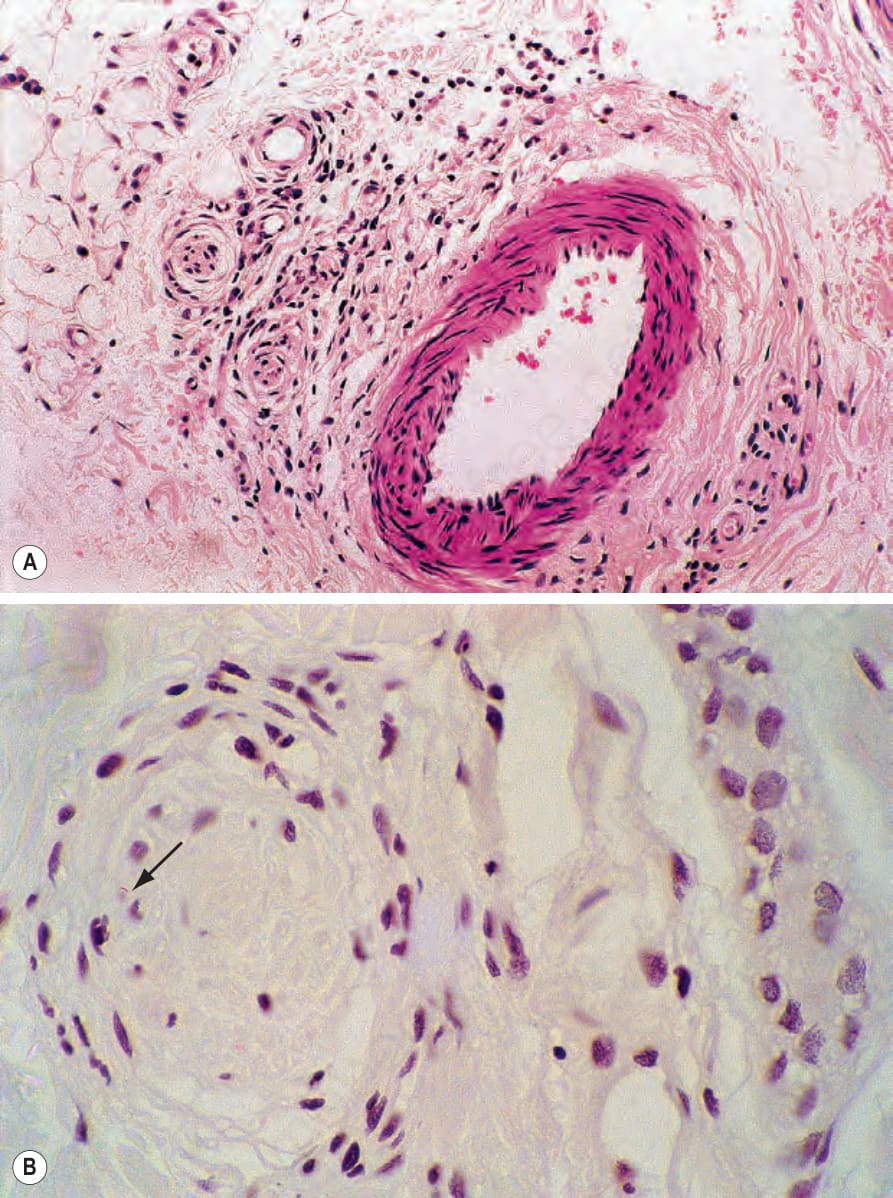
Fig. 18.213 Indeterminate leprosy: (A) the inflammation involves the small nerve trunks; (B) a Wade-Fite reaction may reveal one or two bacilli (arrowed). By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.
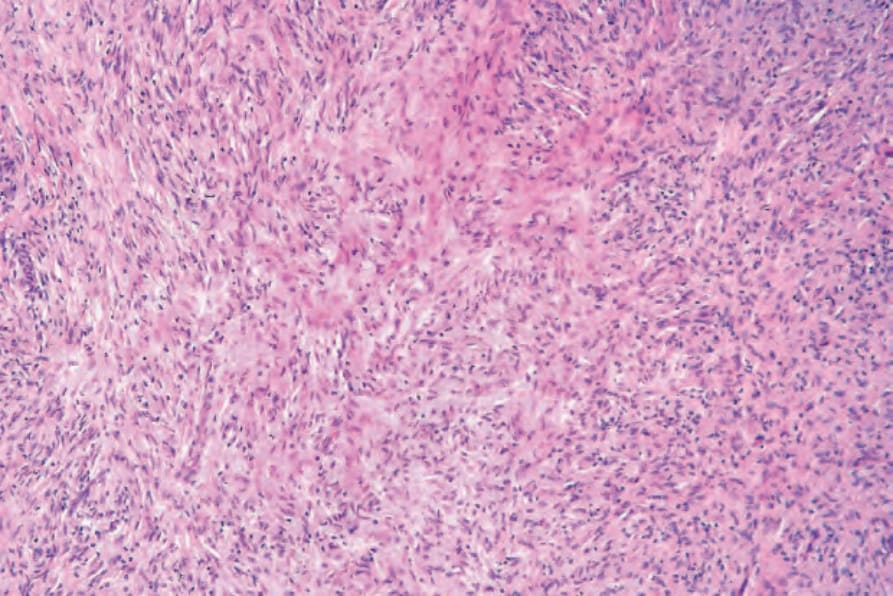
Fig. 18.214 Histoid leprosy: in this field appearances are highly suggestive of a fibrohistiocytic tumor. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.
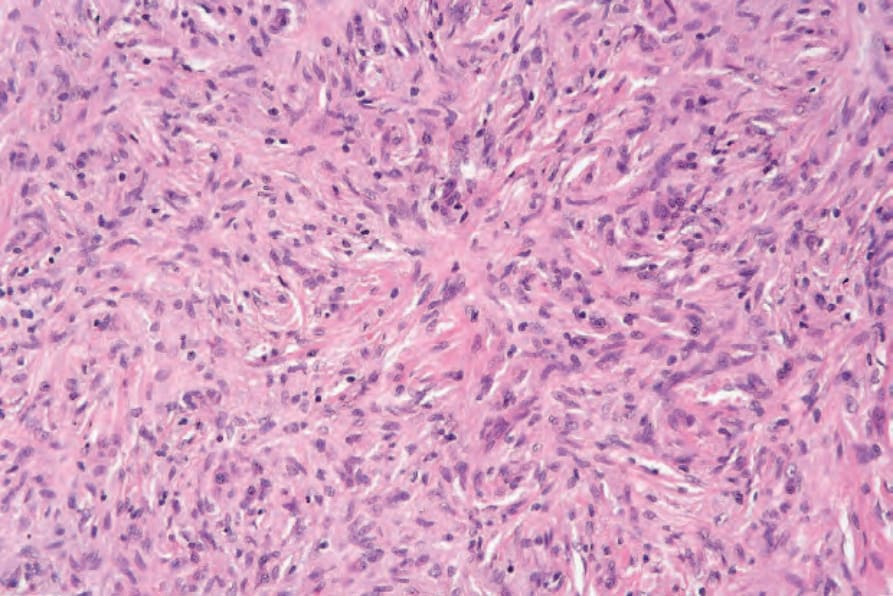
Fig. 18.215 Histoid leprosy: there is a well-developed storiform pattern. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.
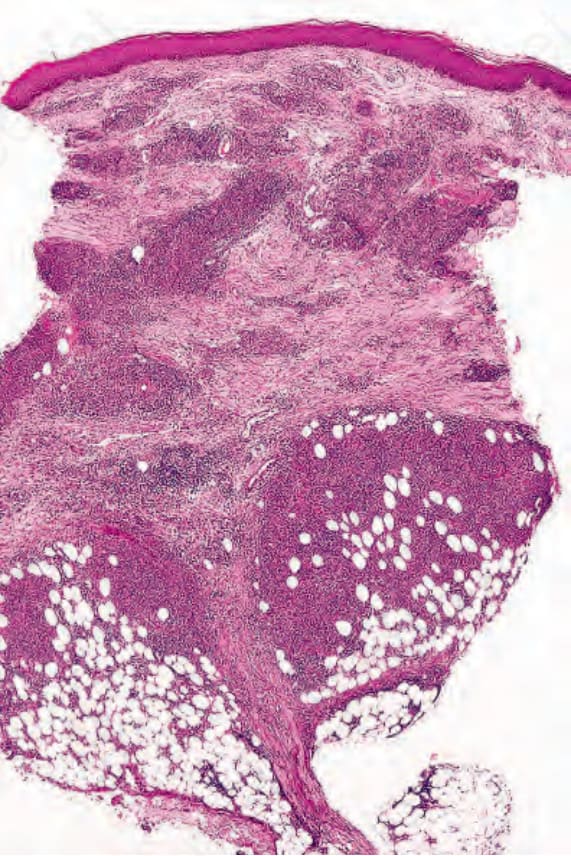
Fig. 18.216 Erythema nodosum leprosum: an intense inflammatory cell infiltrate outlines the dermal vasculature and extends into the subcutaneous fat.
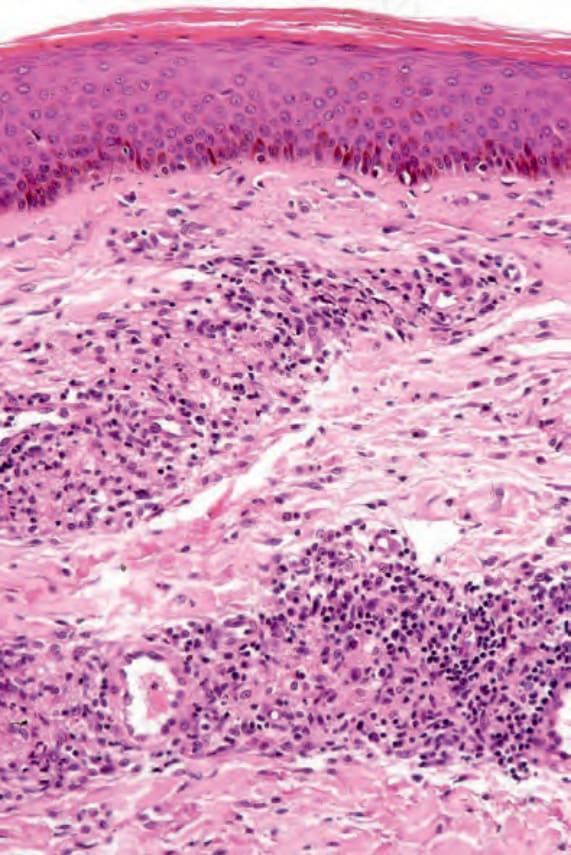
Fig. 18.217 Erythema nodosum leprosum: note the perivascular lymphocyte and histiocyte infiltrate.
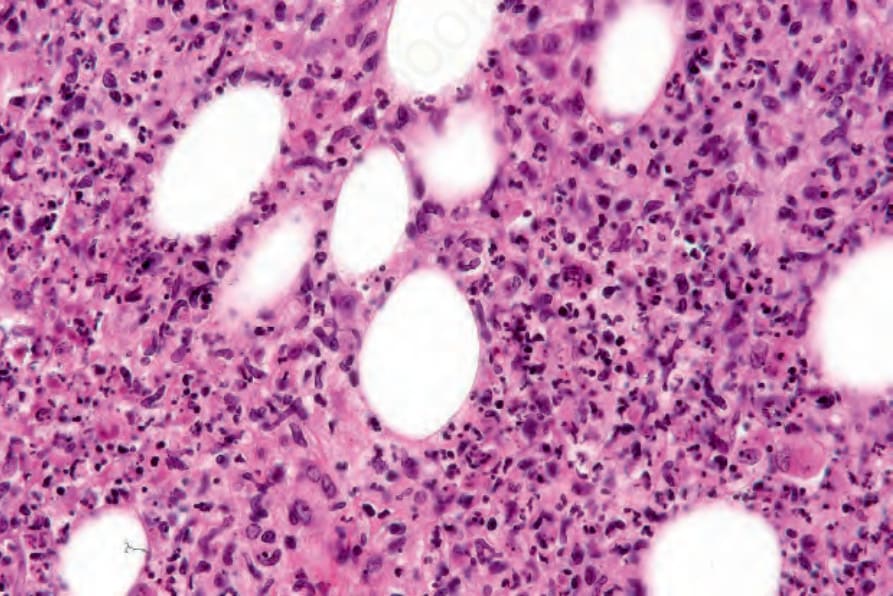
Fig. 18.218 Erythema nodosum leprosum: numerous polymorphs are intermingling with the Lepra cells.
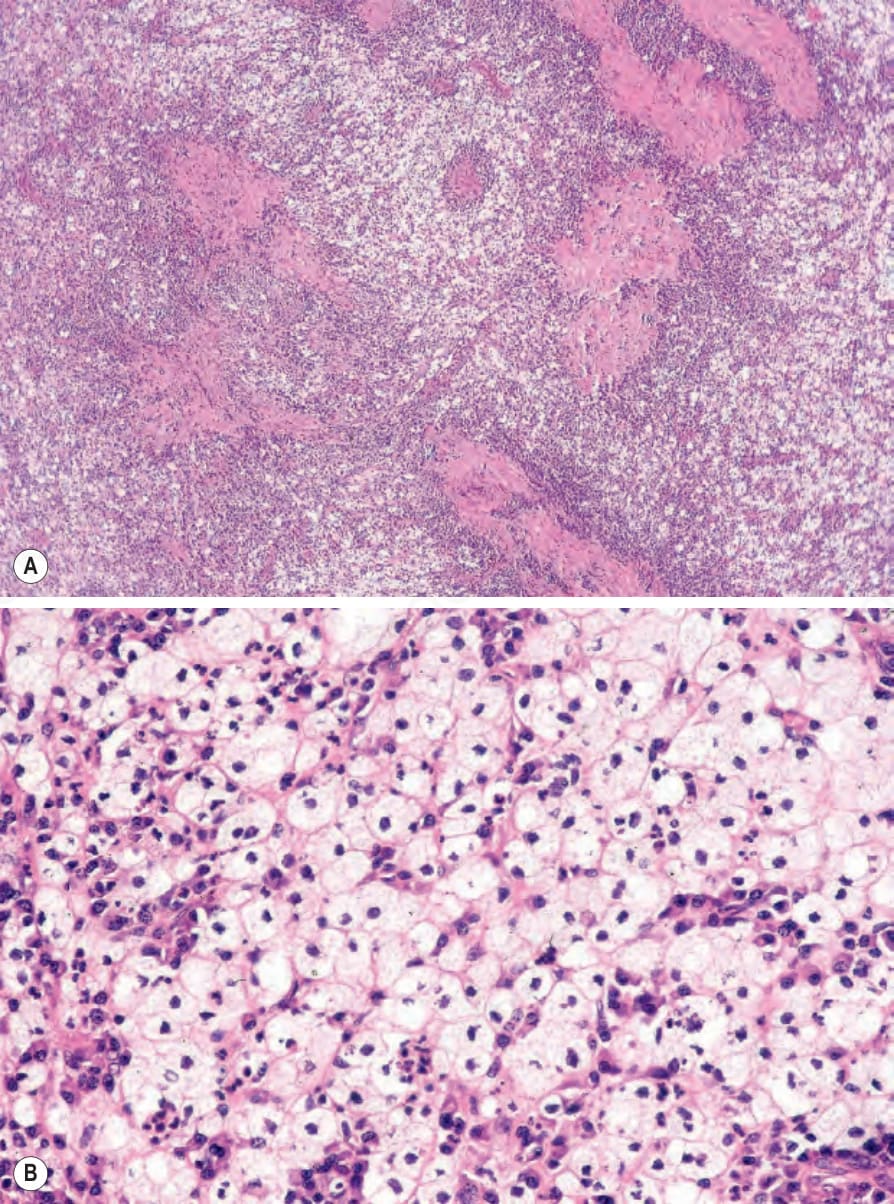
Fig. 18.220 (A, B) Rhinoscleroma: in addition to lymphocytes and numerous plasma cells, foamy macrophages (Mikulicz cells) are present.
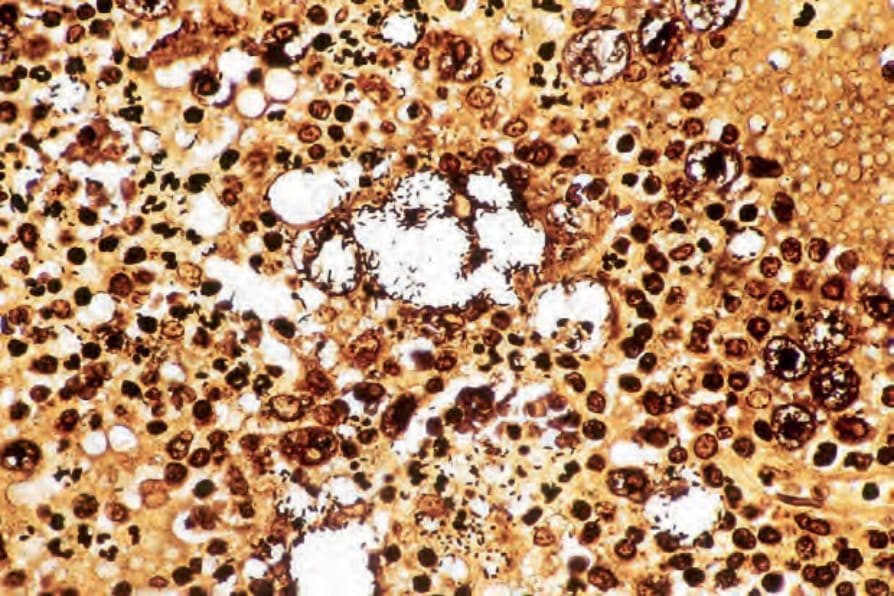
Fig. 18.221 Rhinoscleroma: numerous organisms are revealed by the Warthin-Starry reaction. By courtesy of S. Lucas, MD, Institute of Dermatology, London, UK.