Leprosy
Leprosy
Clinical features Mycobacterium leprae is the bacillus traditionally recognized as causing leprosy (Hansen disease), and until recently could only be cultured in experimental animals, particularly the nine-banded armadillo. It is an obligate intracellular, Gram-positive, weakly acid-fast organism. A major recent development, however, has been the discovery of a second etiological agent of leprosy – M. lepromatosis. The latter is regarded as a species distinct from M. leprae based on an overall 7.4% genomic difference between the respective organisms.1
Leprosy is found worldwide, due to extensive traveling and migration, but is endemic in the tropics.2–5 Recent decades have seen a dramatic decrease in the global disease burden from more than 5 million people in the mid-1980s to around 800 000 by the mid-1990s. More than 250 000 new cases were detected in 2006, a decrease of more than 13% when compared
B
with 2005. The global registered prevalence of leprosy was around 224 000 at the beginning of 2007.6–9 The estimated global prevalence of the disease was around 210 000 in 2015, indicating the number of cases worldwide has plateaued over the past decade.10 However, these data fall short of the WHO’s target for elimination of the disease. Leprosy continues to be a leading cause of infection-related morbidity in many of the 136 countries where it is endemic, despite advances in effective multidrug treatment over the past three decades.10–12
Although the disease has been recognized for many centuries and its main causative organism, M. leprae has been known for more than 100 years, many aspects of the pathogenesis remain unclear or have only recently been elucidated. Leprosy continues to present challenges to diagnosticians, epidemiologists, and pharmacologists alike.
897 Leprosy
M. lepromatosis is now recognized as the species responsible for a unique, severe form of leprosy endemic to Mexico and Costa Rica, referred to as diffuse lepromatous leprosy (DLL). It was initially discovered in fatal cases of DLL in 2008.1,13 Subsequent studies, however, revealed that M. lepromatosis was not only the cause of LL other than DLL in these endemic areas, but was also implicated in other clinical forms of leprosy. M. lepromatosis, therefore, appears to be the dominant cause of leprosy in Mexico. It may coexist with M. leprae in endemic areas, and dual infection with both species may also occur in some patients.1,14 Additional cases of M. lepromatosis infection were later documented in Canada, Singapore, Brazil, and Myanmar.1,14–16
The complexity of the presentation is related intimately to the varied host immunological responses. The incubation period may be as short as 1–2 years, but is usually 3–5 years, and may be 10 years or more. The ability to culture infected macrophages isolated from patients with multibacillary leprosy holds promise for the ex vivo study of M. leprae and its interaction with its host.17
The Ridley & Jopling classification system devised in 1960s is still widely used, and defines the leprosy spectrum based on clinicopathological and immunological criteria.18 There are two extreme modes of presentation:
• the polar tuberculoid form, tuberculoid leprosy (TT),
• the polar lepromatous form, LL.
• Between these are:
• borderline tuberculoid leprosy (BT),
• borderline lepromatous leprosy (BL),
• borderline leprosy (BB) occupying an intermediate position.2–5,18
Tuberculoid leprosy TT is associated with high resistance to the lepra bacillus, but in the lepromatous form resistance to the lepra bacillus is low.4,5,19
TT occurs in individuals with good cell-mediated immunity, but low antibody titers to M. leprae. It appears as localized, sometimes single, asymmetrical truncal or limb lesions. The lesion is typically an erythematous plaque with raised margins and a flat hypopigmented center (Fig. 18.190). Sensory impairment is invariable because of associated involvement of nerves by the bacilli; these nerves may be palpably thickened. Alternatively, the skin lesion may be an erythematous macule, hypopigmented in dark skins. Sometimes the skin is not involved primarily, cutaneous manifestations being seen as a result of minor trauma associated with anesthesia from the neural lesion. M. lepromatosis has been detected in some cases.1
of macules, papules, and plaques may be present at one time, characteristically sparing the axillae, groins, and perineum. These lesions become anesthetic due to widespread neural involvement with resultant claw hand and foot drop (Fig. 18.193).
A rare phenomenon occurring in patients with LL is the development of numerous histiocytoma-like lesions: the histoid variant (Fig. 18.194).21–24 Large cutaneous and subcutaneous nodules and plaques, sometimes measuring in excess of 3 cm in diameter have been described.25–27
Lepromatous leprosy LL is a systemic disease that occurs in patients with poor cell-mediated immunity to M. leprae, but with higher levels of antibodies. The cutaneous lesions are multiple, symmetrical, and may affect the whole skin, giving a sclerodermatous appearance (diffuse or Lucio-type leprosy). It is in this severe diffuse form of LL in particular that M. lepromatosis has been implicated.1,13,20 The more conventional lesions of LL are typically firm and nodular and are concentrated on the face and backs of hands, facial lesions being associated with hair loss round the eyes (Figs 18.191 and 18.192). The distribution of the lesions is said to be favored by lower skin temperature. The mucosa of the nose is characteristically involved and becomes hyperemic with frequent epistaxes. The nasal cartilages and bone may be affected, and collapse can result in a picture similar to the saddle nose of congenital syphilis. A variety
Borderline leprosy Lesions in BT, BL, and BB manifest in a form intermediate between the polar forms TT and LL (Figs 18.195–18.197). The lesions are fewer in number and less symmetrically distributed than in LL, and there is less localization and nerve involvement than in TT. There is, however, a continuous spectrum and individual patients may downgrade to more closely resemble LL or upgrade toward the tuberculoid pole.
Lepra reactions Type I Lepra (reversal) reactions, which usually develop in BL patients, are associated with an upgrading to a more resistant tuberculoid pole of the spectrum and the development of a positive Mitsuda (lepromin)
898 Infectious diseases of the skin
reaction.4,28,29 Patients therefore have developed an improved immunological reaction. Less often, type I reactions may be associated with downgrading. They may be associated with treatment, and consequently are characterized by an accelerated destruction of bacilli. Type I Lepra reactions are also associated with pregnancy, stress, and intercurrent infections. The upgrading causes marked inflammatory changes within the skin: nerve lesions manifest as nerve swelling and pain; cutaneous lesions may become tender and edematous with an increased cellular infiltrate (Fig. 18.198).4
Type II reaction, also known as erythema nodosum leprosum (ENL), occurs in LL and BL, usually during treatment. It may also be provoked by physical or mental stress, injury, other infections, vaccinations, or pregnancy.4,30–32 There appears to be a direct relationship between an increasing
899 Leprosy
A
B
lesions have been reported.35–38 ENL may also occur in patients with leprosy caused by M. lepromatosis.1,39
Lucio phenomenon Lucio phenomenon (erythema necroticans) is seen almost exclusively in Mexican and Central American patients who present with untreated, diffuse, non-nodular LL (pure and primitive DLL; diffuse leprosy of Lucio and Letapí). As stated earlier, M. lepromatosis is now recognized as the agent responsible for this severe, diffuse form of LL. There is associated hemorrhagic infarction and epidermal necrosis (Fig. 18.200).31,40–44 Unsurprisingly, M. lepromatosis has recently been linked to Lucio phenomenon.39,45 Lesions, which are initially macular, then soon break down to become irregular jagged ulcerations, which heal to leave irregular atrophic scars. The extremities are most commonly affected. Although Lucio phenomenon, like ENL, was considered to be mediated by immune complexes, this concept has since been challenged. It has been suggested that the triggering event is thrombotic vascular occlusion secondary to massive invasion of vascular endothelial cells by the bacilli, resulting in necrosis.44 In one retrospective study of 12 cases, however, a necrotizing panvasculitis was evident in all cases.46 A recently reported case with associated antiphospholipid syndrome
bacterial index and the risk of developing ENL. Increasing age, on the other hand, has been found to have an inverse relationship with ENL. The reaction may occur prior to, during, or after the introduction of multidrug therapy.33 The changes of ENL are believed to be due, at least in part, to immune complex deposition in vessels following the release of bacterial antigens in patients who have high levels of antibodies. Both immunoglobulins and complement have been identified in blood vessel walls. Delayed hypersensitivity mechanisms, however, are also thought to have a pathogenetic role. In ENL there are, therefore, increased numbers of Th cells, and an increased lesional helper/suppressor T-cell ratio is characteristic.31 Studies performed on lesional tissue have confirmed a preponderance of CD4+ T-cells and a Th1-type immune response.34 The symptoms are nocturnal pains, mainly of the face, thighs, and arms. Lesions include tender erythematous or deep purple nodules with fever and painful nerve swelling, swollen joints, myositis, painful fingers, iritis, lymphadenitis, glomerulonephritis, and epididymo-orchitis (Fig. 18.199).31 Cases with bullous skin
900 Infectious diseases of the skin
showed thrombotic luminal occlusion of dermal vessels in the absence of associated vasculitic changes.47
Indeterminate leprosy Indeterminate leprosy is an early form of leprosy, which often resolves spontaneously.48 However, in 25% of patients, evolution to one of the determinant types occurs. It appears as poorly defined areas of slight hypopigmentation or erythema, without systemic or neural changes. The condition is only likely to be recognized readily in endemic areas where there is a high awareness of leprosy. It must be carefully distinguished from other dermatoses.
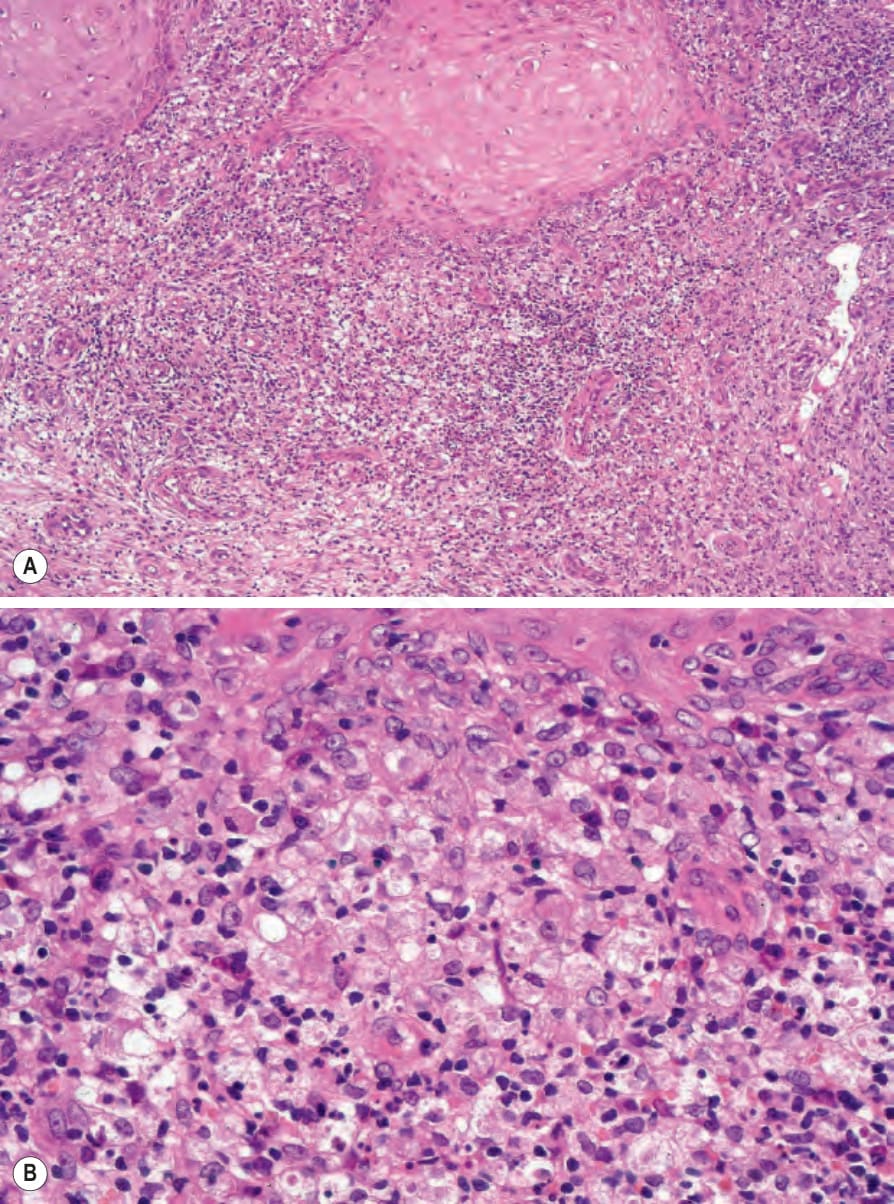
Fig. 18.189 (A, B) Mycobacterium avium intracellulare: in this variant, the infiltrate typically consists of histiocytes, lymphocytes, and neutrophils. Bacteria are often numerous.

Fig. 18.190 Tuberculoid leprosy: note the hypopigmentation and erythema. By courtesy of B. Al-Mahmoud, MD, Doha, Quatar.

Fig. 18.191 Lepromatous leprosy: numerous nodules are present on the face. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.

Fig. 18.192 Lepromatous leprosy: note the symmetry and characteristic loss of the eyebrows. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.

Fig. 18.193 Lepromatous leprosy: these hands show loss of the digits and trauma-related ulcers due to gross nerve damage. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.

Fig. 18.194 Histoid leprosy: these numerous brown papules and nodules may be histologically mistaken for a ‘fibrohistiocytic’ tumor if the clinical information is not available. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.

Fig. 18.195 Borderline tuberculoid leprosy: an early hypopigmented macule. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.

Fig. 18.196 Borderline tuberculoid leprosy: note the ulceration and muscle wasting due to median and ulnar nerve involvement. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.

Fig. 18.197 (A, B) Borderline lepromatous leprosy: there are gross infiltrated erythematous plaques with well-defined borders. (A) By courtesy of S. Lucas, MD, Institute of Dermatology, London, UK; (B) by courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.

Fig. 18.198 Type I Lepra reaction: note the unilateral edema and intense erythema. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.

Fig. 18.199 Erythema nodosum leprosum: note the erythematous nodules on the dorsal aspect of the forearms and shins. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.

Fig. 18.200 Lucio phenomenon: note the multiple infarcted cutaneous nodules, which have developed against a background of diffuse lepromatous leprosy. By courtesy of R. Arenas, MD, and J.C. Salas, MD, Monterrey, Mexico.
Fig. 18.203 Tuberculoid leprosy: lymphocytes are present in addition to giant cells and granulomata.
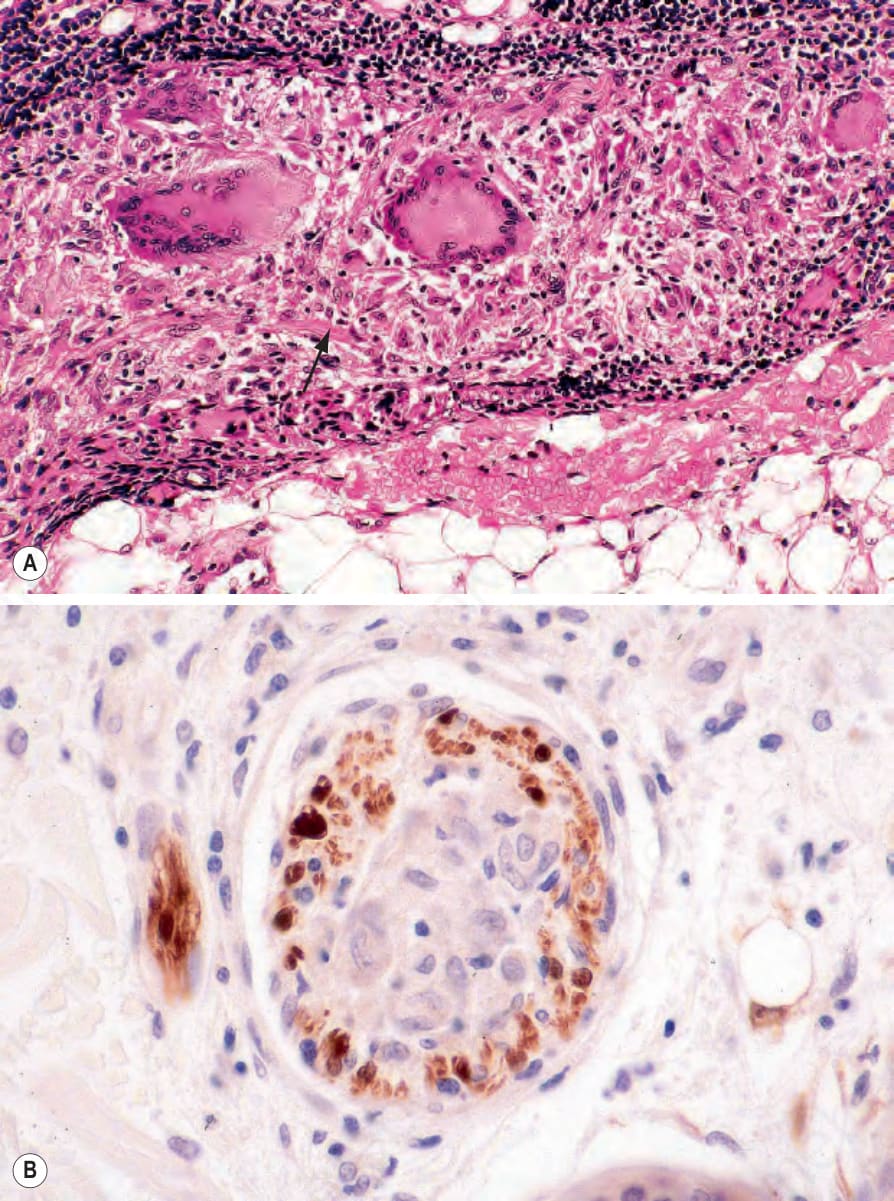
Fig. 18.204 Tuberculoid leprosy: (A) this small nerve is almost completely replaced by the granulomatous infiltrate; the residual nerve tissue is arrowed; (B) S100 protein immunohistochemistry is invaluable in identifying damaged nerves.
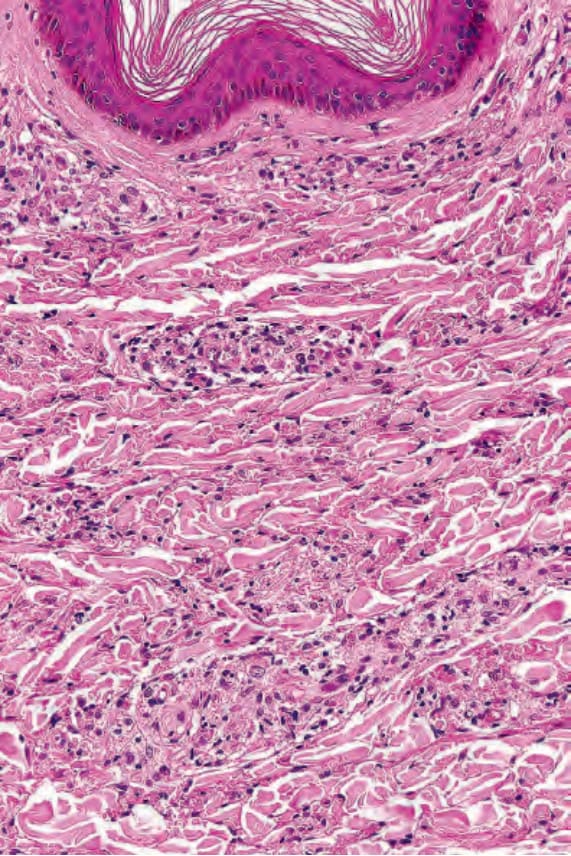
Fig. 18.206 Lepromatous leprosy: a Grenz zone of sparing of the papillary dermis is characteristic.
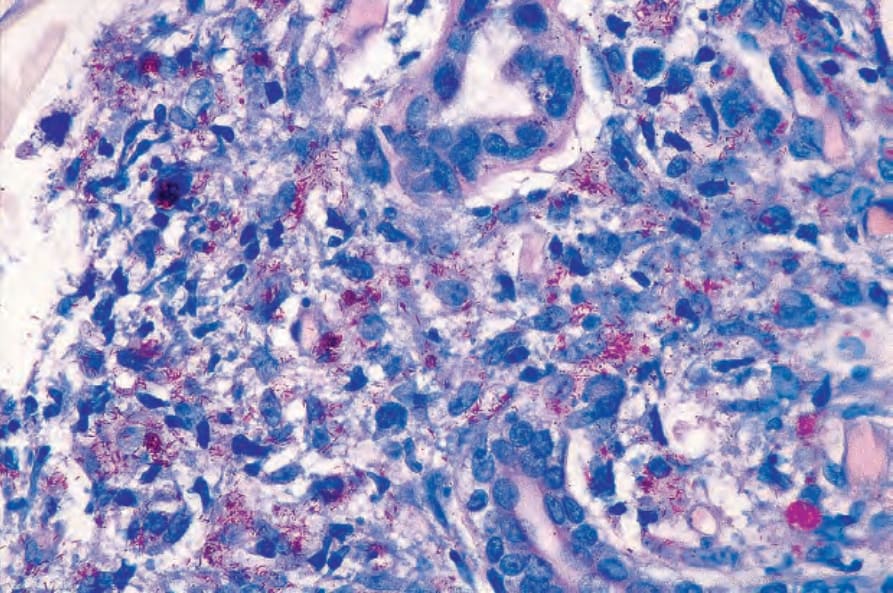
Fig. 18.211 Subpolar lepromatous leprosy: leprosy bacilli are numerous (Wade-Fite).
epithelia.64 Inoculation leprosy is a rare phenomenon acquired through skin tattooing.65
The responses of those that are infected may be determined by a genetic predisposition, as suggested by associations with human leukocyte antigen (HLA) class II antigens, including HLA DR2 and DR3 in tuberculoid leprosy, and HLA DQ1 in LL.18 Genome-wide association studies have uncovered a number of candidate genes which may confer an increased susceptibility to the disease, including genes whose product is directly involved in the host response to the organism. Among these are polymorphisms in the promoters of the genes encoding TNF-α and IL-10.18,66 The MRC1 gene on chromosome 10p13, for example, has been of particular interest.18 A noteworthy aspect uncovered by these studies is that some leprosy susceptibility genes are shared with Crohn disease and Parkinson disease.62 Reversal reactions appear to be associated with variations in the TLR1 AND TLR2 genes.18
The Mitsuda reaction (intradermal injection of armadillo-derived Lepra bacilli) has proved useful for classification purposes.5 Tuberculoid patients develop a granulomatous response; lepromatous patients do not (Fig. 18.201).4
Although leprosy has been reported in patients infected with HIV, current evidence suggests that M. leprae is not an opportunistic pathogen in these individuals.49–51 There have, however, been a number of reports of leprosy occurring as a manifestation of IRIS following the initiation of highly active ART in HIV-infected individuals.52–56 Leprosy is only rarely encountered in immunosuppressed organ transplant recipients.57
Leprosy patients with chronic cutaneous ulcers (especially plantar lesions) are at increased risk for the development of squamous cell carcinoma.58,59
Pathogenesis and histologic features The varied clinical manifestations of leprosy are the result of a number of factors, including the host’s immune response, the mode of infection, and certain genetic factors.18,60–63 It was long assumed that transmission of leprosy was by long-term close direct skin contact, but this can be seriously questioned as there is no evidence that infection can occur through intact skin. LL is far more infective than other forms, and the nasal mucosa and nasal secretions of patients with LL are heavily infected with bacilli. This is a most important source of infection, but it is not clear that the route of transmission is via the lungs or gastrointestinal tract, even though inhalation of droplets and ingestion of bacilli do occur. Lactating mothers with LL produce high counts of bacilli in milk and yet do not appear to spread leprosy to their babies. It seems most likely that infection in leprosy occurs by a combination of nasal discharge and digital impregnation of the skin, as bacilli can be carried under the nails and inoculated into the skin by scratching. One study revealed that untreated patients with multibacillary leprosy may shed organisms into the environment via their skin and nasal
Leprosy can be regarded as either paucibacillary (localized) or multibacillary (disseminated), with vigorous Th1 (cell-mediated) and Th2 (humoral) immune responses characterizing the former and the latter, respectively.67 In tuberculoid lesions, there is an efficient granulomatous macrophage response, associated with a preponderance of Th (CD4+) cells over T-suppressor cells (CD8+) in an approximate ratio of 2:1, and no antibody production. There is associated elimination of the bacteria, which are therefore difficult to find in tuberculoid lesions. The tuberculoid response is therefore characterized by a persistent or chronic delayed hypersensitivity reaction, with a Th1 immune response and release of IFN-γ, IL-2, and TNF-α. A Th2 response characterizes multibacillary leprosy, with high levels of IL-4, IL-5, and IL-10, and low levels of IFN-γ.4,17,18,61 In lepromatous lesions T-suppressor cells are more numerous and IL-2 producing cells are scarce, whereas they are 10 times more common in TT. One explanation for the different response suggests that Th cells are defective or absent in individuals who develop LL. An alternative theory suggests that T-suppressor cells are activated by the leprosy bacilli in patients of certain HLA-DR types. It is proposed that this represents a response to PGL-I, which is peculiar to the cell envelope of the leprosy bacillus. The T-suppressor cells effect a reduction of Th cells reactive to M. leprae. In this way, the T-suppressor and Th theories are not incompatible. The variable immune response to the Lepra bacillus is manifest
901 Leprosy
in the wide variety of clinical manifestations in leprosy.18,68 Other genetic factors including Lewis factor and natural resistance-associated macrophage protein 1 (NRAMP1) may also play a role.60 BCG vaccination may play a beneficial role in the prevention of leprosy.67,69
In LL there is an inability to develop a significant T-cell-mediated delayed hypersensitivity reaction to the leprosy bacillus.4 The high level of antibodies in LL appear to have no beneficial effect, but are relevant to the development of the immune complex-mediated ENL lesions (see above). Lucio phenomenon, in which purpura and leg ulcers develop, was thought to involve a similar immune complex-mediated mechanism to produce episodes of necrotizing vasculitis in this diffuse type of leprosy. Others, however, have since suggested that direct invasion of vascular endothelium by large numbers of bacilli, with subsequent thrombosis of vessels, is the major factor in the evolution of this reaction.44 Antiphospholipid antibodies may also play a role.47,70
Histologically, TT is characterized by an epithelioid histiocyte response around small cutaneous nerves (Figs 18.202–18.204). It may be entirely confined to the immediate vicinity of nerves in highly immune patients, but it often extends into the adjacent dermis. When there are clinical cutaneous lesions, the infiltrate involves the papillary dermis up to the epidermis. In contrast, BT and more lepromatous forms have a preserved Grenz zone in the papillary dermis. Tuberculoid lesions usually contain a number of Langhans giant cells, but necrosis is not a feature. Bacilli are so scarce in tuberculoid lesions that they are usually not identified; they are present in increasing numbers in variations closer to the lepromatous type of response. Distinguishing TL from other forms of granulomatous infiltrate of the skin is dependent on noting the association with nerves, which often gives the granuloma a serpentine shape. In addition, there are numerous lymphocytes, largely Th type, which may infiltrate the nerves in highly immune cases; the lymphoid infiltrate may be intense and extensive.
A
In LL, as in TL, the macrophage is the most important cell, but it is not arranged in discrete granulomata nor clearly related to nerves. Rather, macrophages are found in poorly circumscribed masses in the dermis with few, if any, lymphocytes (Figs 18.205 and 18.206). Those lymphocytes that are present are T-suppressor cells. The macrophages are inert and often vacuolated or foamy (Fig. 18.207. They may be distended with large groups
B
902 Infectious diseases of the skin
eccrine secretory and ductal cells.72 Exceptionally, clumps of bacilli may even be encountered in epidermal keratinocytes.73
Plasma cells are rarely seen in leprosy. They may, however, be found in subpolar LL, which clinically lies between BL and polar LL (Figs 18.209–18.211).
In borderline leprosy, perineural fibrosis with a lamellar or ‘onion skin’ pattern may be seen. Borderline leprosy shows increased circumscription of the granulomatous response, more lymphocytes, and more relation to nerves as it approaches the polar tuberculoid form.
(or globi) of leprosy bacilli. These give the cytoplasm a grayish tinge on staining with H&E; the bacilli are revealed more clearly with a modified Ziehl-Neelsen stain (Wade-Fite) (Fig. 18.208). The bacteria are present in large numbers of cutaneous nerves and are also seen in that site in the borderline forms of leprosy.71 Bacilli may also be present in the endothelium and media of small and large vessels, in arrector pili muscles, and in the
Indeterminate leprosy shows only a scanty superficial and deep lymphohistiocytic infiltrate in the dermis, with some tendency to localization around appendages (Fig. 18.212). Bacilli are infrequent, but scantily present in nerves (Fig. 18.213). Mast cells are increased.74 S100 protein immunohistochemistry is a useful means of identifying dermal nerves and foci of nerve damage in skin biopsy specimens.75,76
Histologically, in most instances Lucio phenomenon is characterized by the features of a leukocytoclastic vasculitis and epidermal infarction.31,44,46,77 Severe passive venous congestion of the superficial veins is common.31 Occasionally, however, some vessels are thrombosed and there is endothelial cell proliferation and swelling, with distortion, narrowing, and luminal obliteration.40,46,77,78 The medium-sized arteries in the deep dermis and superficial subcutis show mural infiltration by clusters of macrophages containing large
903 Rhinoscleroma
be seen.71 ENL is characterized by an inflammatory cell infiltrate in the dermis and adjacent subcutaneous fat (Figs 18.216–18.218). In addition to Lepra cells, large numbers of neutrophils are typically present, and there is often an acute vasculitis (Fig. 18.219).30,34,71,79 Bullous lesions are characterized by dermal edema.25 Organisms are demonstrable within capillary endothelium.38,44
Molecular techniques (PCR) may prove useful in confirming the diagnosis of leprosy, especially in paucibacillary forms or when organisms are not readily apparent in sections stained with the Wade-Fite method.80–82
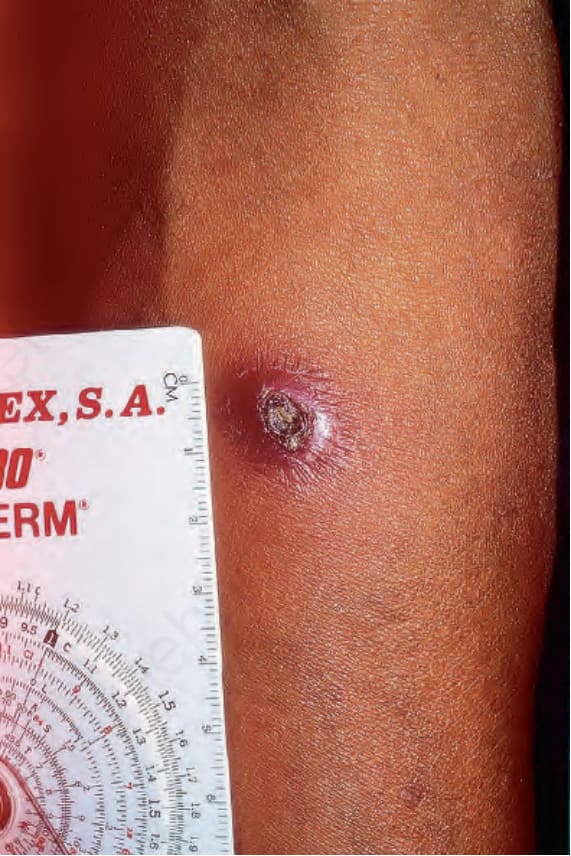
Fig. 18.201 Mitsuda reaction: this is positive in a patient with tuberculoid leprosy. By courtesy of R. Arenas, MD, and J.C. Salas, MD, Monterrey, Mexico.
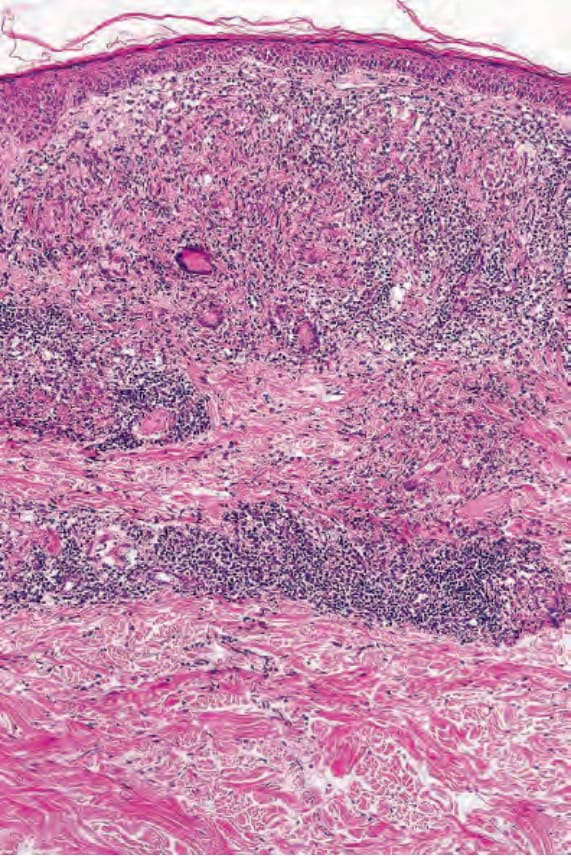
Fig. 18.202 Tuberculoid leprosy: there is extensive infiltration of the dermis and subcutaneous fat by noncaseating granulomata.
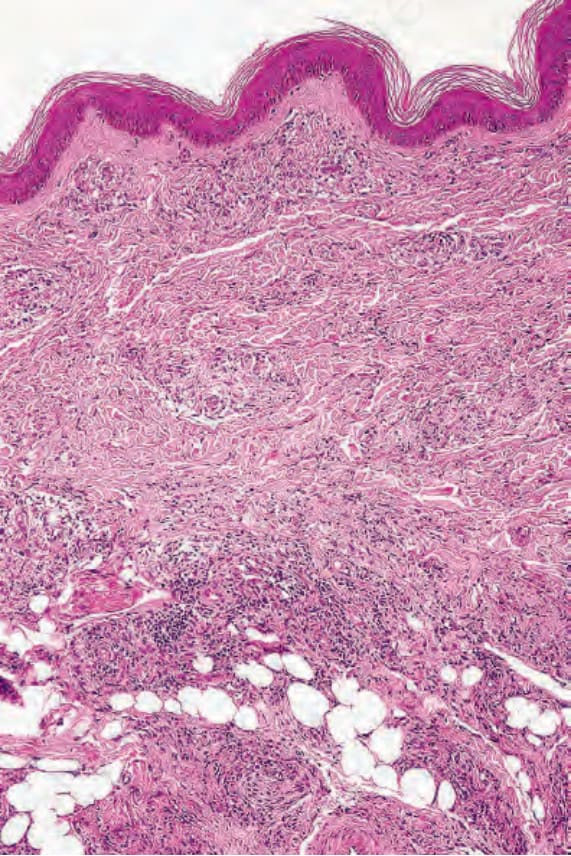
Fig. 18.205 Lepromatous leprosy: there is infiltration of the dermis by large numbers of histiocytes.
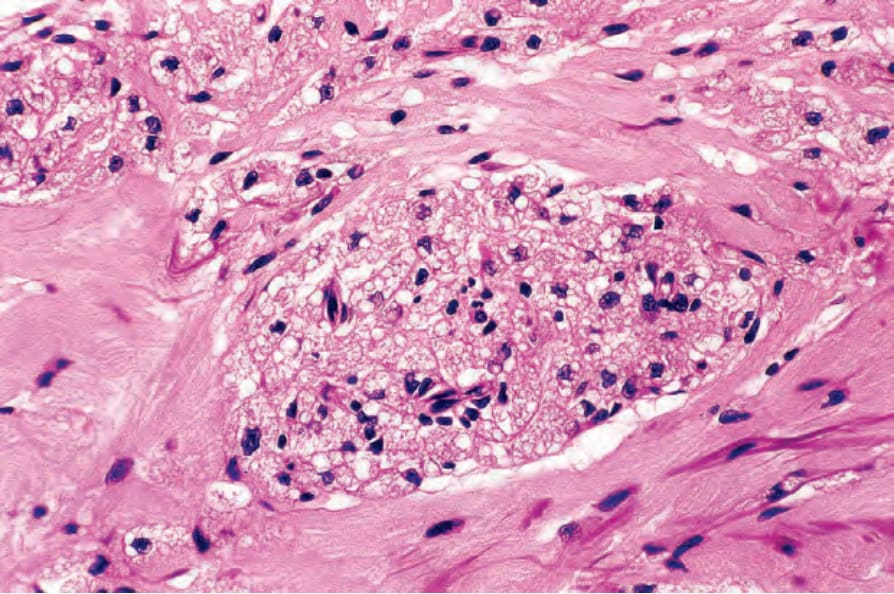
Fig. 18.207 Lepromatous leprosy: the cytoplasm of the histiocytes is bubbly and has a grayish hue.
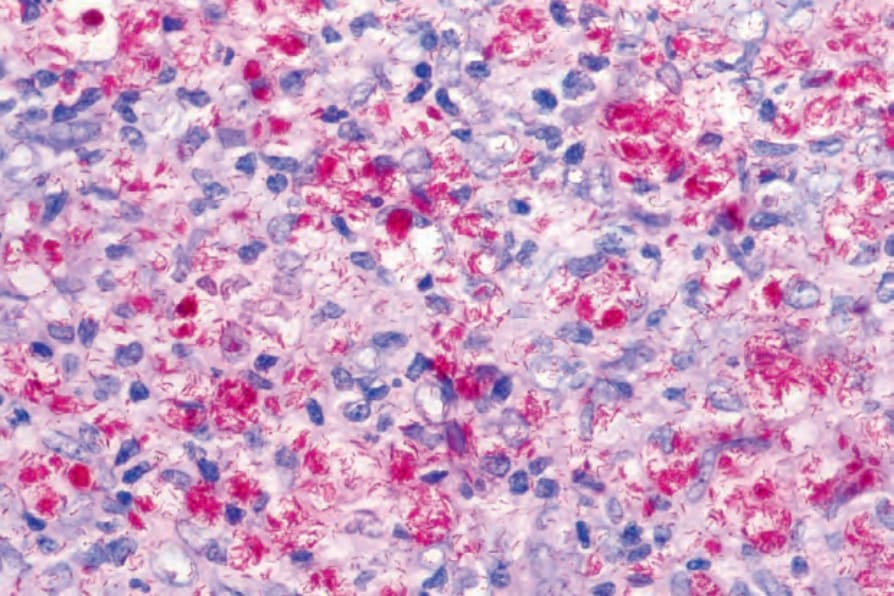
Fig. 18.208 Lepromatous leprosy: large numbers of bacilli are present; note the globi (Wade-Fite).
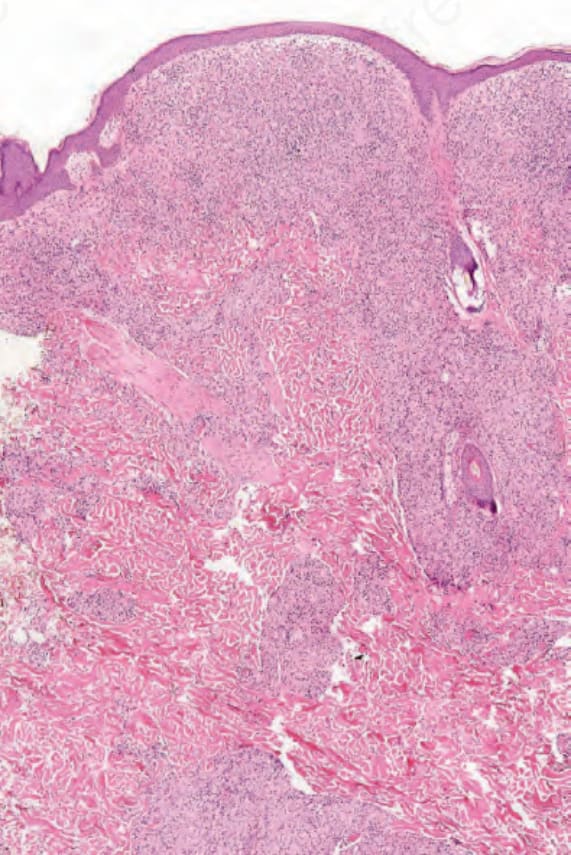
Fig. 18.209 Subpolar lepromatous leprosy: there is a dense dermal infiltrate. A Grenz zone is present.
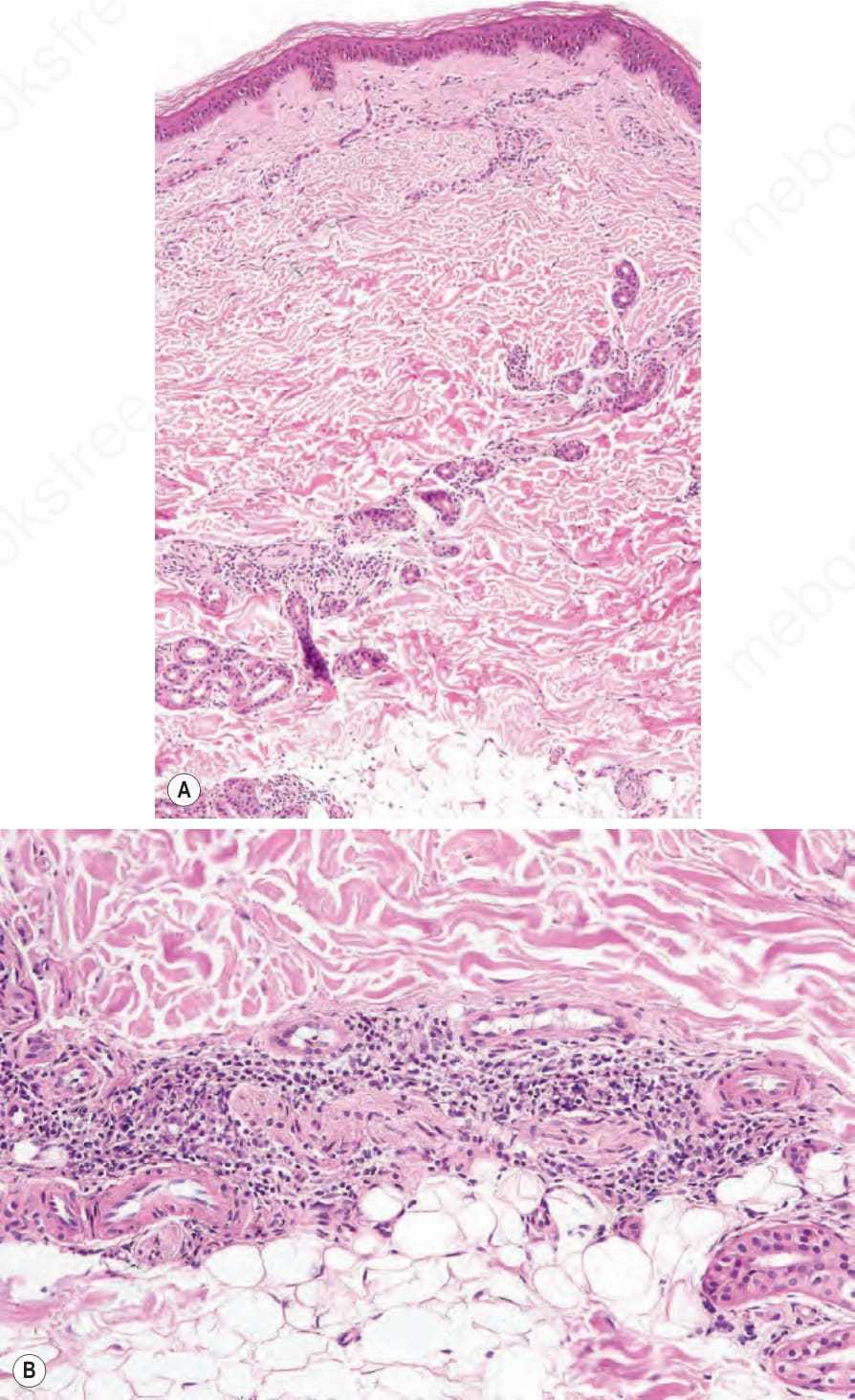
Fig. 18.212 (A, B) Indeterminate leprosy: a perivascular chronic inflammatory cell infiltrate is present in the deep dermis. Diagnosis depends on a high index of suspicion.
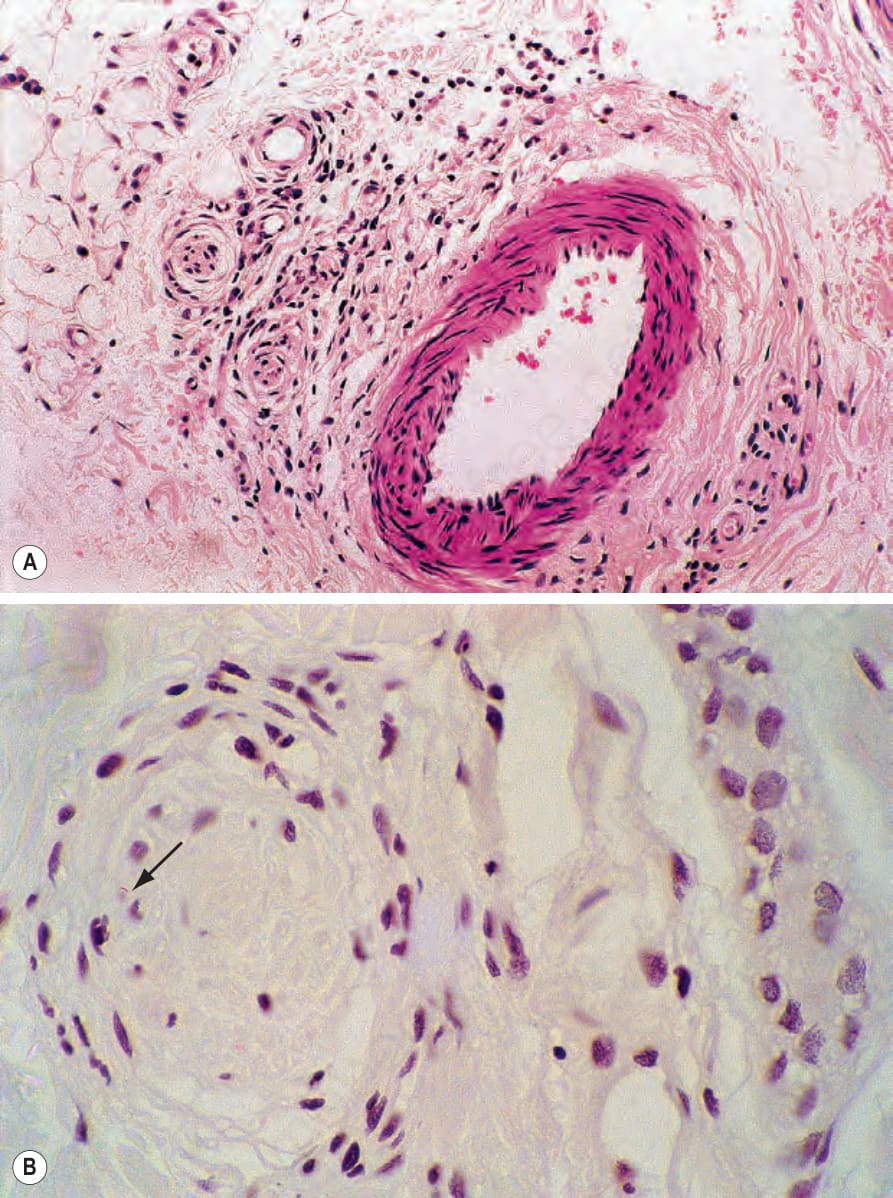
Fig. 18.213 Indeterminate leprosy: (A) the inflammation involves the small nerve trunks; (B) a Wade-Fite reaction may reveal one or two bacilli (arrowed). By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.
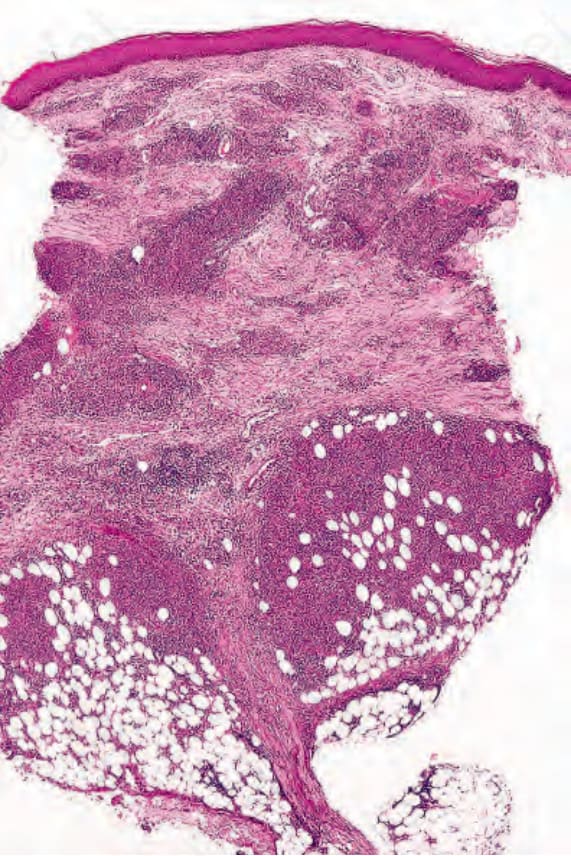
Fig. 18.216 Erythema nodosum leprosum: an intense inflammatory cell infiltrate outlines the dermal vasculature and extends into the subcutaneous fat.
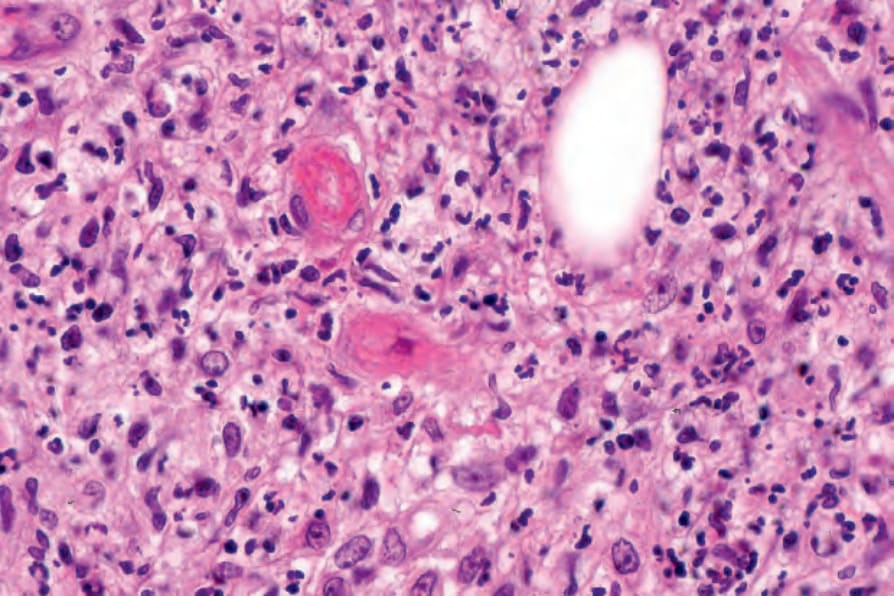
Fig. 18.219 Erythema nodosum leprosum: several small vessels show fibrinoid necrosis. This type II reaction develops on the basis of an immune complex-mediated vasculitis.