Tuberculids
Tuberculids
Clinical features A tuberculid is a cutaneous immunological reaction to the presence of tuberculosis, which is often occult, elsewhere in the body.1–3 By definition, special stains and cultures for tubercle bacilli from tuberculids are negative. Although tuberculids are rare in Western countries, they are still important conditions in developing countries where tuberculosis is a common disease.3–5
Tuberculids may be papular or nodular and can be separately classified on that basis, but variations and combinations of those features may be seen and are only valid descriptively.
One variety of papular tuberculid is the papulonecrotic tuberculid. This chronic condition presents as recurring crops of flesh-colored, erythematous,
or darkish red papules, most often on the ears and the limbs and in particular on extensor aspects around the elbows and knees (Figs 18.167 and 18.168).4–9 Lesions may occur widely or present in isolated sites.7,10 The papules may become pustular, ulcerate, or develop crusts. They are often symmetrically distributed.11 Genital involvement may occasionally occur.7 Uncommonly, the papules may assume an MC-like appearance.12 They regress slowly over several weeks, leaving depressed, varioliform scars.11,13 Usually they occur in young people who otherwise often appear rather well. Occasional cases have been reported to progress to lupus vulgaris.3,6
889 Tuberculids
A
Lichen scrofulosorum characteristically presents as yellow or brown asymptomatic follicular papules, less than 3 mm across, on the trunk (Fig. 18.169). These lesions regress slowly and do not leave scars. This uncommon tuberculous reaction usually occurs in children and young adults.8,9,14–17 Lesions mimicking psoriasis or lichen planus have been described.18,19 The eruption is said to be more frequently associated with tuberculous lymphadenitis (cervical, hilar or mediastinal) or osseous tuberculosis than with pulmonary tuberculosis.8,15 The latter observation has not been supported by others.14,15 It has also been reported following BCG vaccination, and in association with underlying M. avium-intracellulare (MAI) infection.8,9
B
Until recently, the only nodular tuberculid that was generally accepted was erythema induratum (Bazin disease, nodular vasculitis). This condition presents as ill-defined nodules on the calves of predominantly young and middle-aged women, characteristically those who are obese, and have erythrocyanotic skin in this area. The lesions may be worse in cold weather, which raises the problem of distinction from pernio. With progression, the nodules eventually form irregular ulcers, which tend to have bluish undermined edges. Resolution is slow but most lesions disappear spontaneously over a few months. Potential sequelae include postinflammatory hyperpigmentation or atrophic scars.8,9
Pathogenesis and histologic features All tuberculids are immunological reactions thought to be due to hematogenously disseminated M. tuberculosis antigens or small numbers of dead bacteria, possibly opsonized. These embolize to produce lesions, particularly in areas of slow circulation. As a result of changes in small dermal vessels (either an Arthus reaction or a lymphohistiocytic vasculitis), degenerative responses develop in the dermal collagen. In the case of papulonecrotic tuberculid, this amounts to frank necrosis. Histologically, the lesions show variable combinations of vasculitis with necrosis, a moderate to intense lymphohistiocytic infiltrate, and granulomatous inflammation.
The term nodular tuberculid has been applied to a rare subset of patients with nonulcerated nodules on the lower legs and in whom the pathological changes are centered on both the dermis and the subcutaneous fat.12,20,21 It has been proposed that this entity represents a hybrid between papulonecrotic tuberculid and erythema induratum of Bazin.20 Rare cases of papulonecrotic tuberculid coexistent with erythema induratum have also been reported.22–25
The terms nodular granulomatous phlebitis of the skin and superficial thrombophlebitic tuberculid have been proposed for an additional type of tuberculid which presents as subcutaneous nodules along the course of a leg vein. There is histologic evidence of granulomatous inflammation centered on the wall of the affected vessel.26,27 This condition should be distinguished from true tuberculous phlebitis as a consequence of miliary tuberculosis.
Papulonecrotic tuberculid, when fully developed, shows cutaneous infarction comprising a necrotic epidermis with ulceration and an underlying V-shaped zone of dermal coagulative necrosis accompanied by a dense chronic inflammatory cell infiltrate with scattered giant cells.4,5,11,13 Necrosis of hair follicles may occur.28 On occasion, a histiocytic palisade has been described, resulting in features reminiscent of granuloma annulare. Neutrophils are generally inconspicuous. Well-formed granulomata can be present in older lesions, but bacilli cannot be identified. Vasculitis may be present.6,9,11 These features can sometimes be histologically confused with pityriasis lichenoides et varioliformis acuta.10,28
In lichen scrofulosorum, a granulomatous infiltrate in which Langhans giant cells are conspicuous is centered around hair follicules and eccrine units (Fig. 18.170). Caseous necrosis is usually absent.4,9
Erythema induratum is indistinguishable from nodular vasculitis. The changes are centered on the subcutis. There is predominantly lobular
890 Infectious diseases of the skin
panniculitis in association with tuberculoid granulomas, areas of caseation necrosis, and variable vascular involvement of mainly the venules and small to medium caliber arteries, including frank vasculitis.5,9,29 Due to the prominent necrosis, the vasculitis is often difficult to identify. The presence of both primary vasculitic changes and granulomatous inflammation suggests that type III and type IV hypersensitivity reactions are important in the latter condition.30
Although acid-fast organisms are not detectable by special stains, and mycobacterial cultures from these lesions invariably are negative, M. tuberculosis DNA has been detected by PCR in a number of cases; this suggests that mycobacterial components are indeed responsible for the pathological manifestations.13,31–33
with cutaneous involvement secondary to intravesical BCG instillation has been reported.20
Histologic features In immunocompetent individuals, skin and lymph node biopsy material may reveal multiple epithelioid cell granulomas with admixed Langhans giant cells and minimal caseous necrosis, with or without concomitant suppuration.15 Conversely, involved tissues obtained from immunosuppressed individuals are characterized by a diffuse infiltrate of plump histiocytic cells, with poorly developed or absent granuloma formation. The cytoplasm of these histiocytes is distended by large numbers of acid-fast M. bovis bacilli (Fig. 18.172).2,10,15 The histologic findings in this latter group are similar at all sites of involvement, including cutaneous, subcutaneous, lymph node, or visceral tissues. The diagnosis may be confirmed by PCR.21,22 A pattern of dermal involvement mimicking granuloma annulare has been reported.13
The validity of the concept of the tuberculids rests on the association with underlying tuberculosis, a strong tuberculin reaction, and an invariable response to antituberculous drugs.
Cutaneous complications of bacille Calmette-Guérin vaccination
Clinical features For almost a century, the BCG vaccine, which employs a live but attenuated form of Mycobacterium bovis, has been administered to newborns for the prevention of tuberculosis. BCG immunization is currently carried out in more than 100 countries worldwide where endemic tuberculosis remains a serious public health problem.1 In recent years, a number of cutaneous and other complications have been recorded, especially in infants with primary immunodeficiency syndromes.2–8 Complications have also been documented in infants and children infected with HIV.9–11 It has been shown that HIV infection leads to severe impairment of the BCG-specific T-cell response during the first year of life.11
Differential diagnosis Mycobacterial culture and PCR studies facilitate distinction between cutaneous, subcutaneous, or disseminated BCG infection in immunocompromised hosts from infection with MAI complex and other nontuberculous mycobacterial infections. The degrading intracytoplasmic organisms contained within macrophages in the subcutaneous nodules of Whipple disease, are PAS-positive but fail to stain with Ziehl-Neelsen method.
Local infection may develop at the vaccination site, with abscess formation (BCGitis).4,6,7 Regional lymphadenitis is another well-recognized complication (Fig. 18.171), and may be accompanied by cutaneous fistula formation or scrofuloderma.2,5,9,12 Disseminated skin lesions may also occur, manifesting with a widespread papular eruption or multiple nodules or abscesses in the skin and even the subcutis.1–6,9,10,13,14 Dissemination of disease (BCGosis) can prove fatal.14,15 Organs that may potentially be involved include the spleen, mesenteric and mediastinal lymph nodes, bone marrow, liver, and lungs.2,9 Other documented cutaneous manifestations include lupus vulgaris, erythema induratum, and papulonecrotic tuberculid-like lesions.16–19 A case
A
B

Fig. 18.167 Papulonecrotic tuberculid: widely distributed small purple papules are present. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.

Fig. 18.168 Papulonecrotic tuberculid: innumerable papules are distributed on the dorsal aspect of the legs. Tuberculids imply an active infection elsewhere in the body. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.

Fig. 18.169 Lichen scrofulosorum: note the numerous tiny papules on the chest and upper abdomen. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.
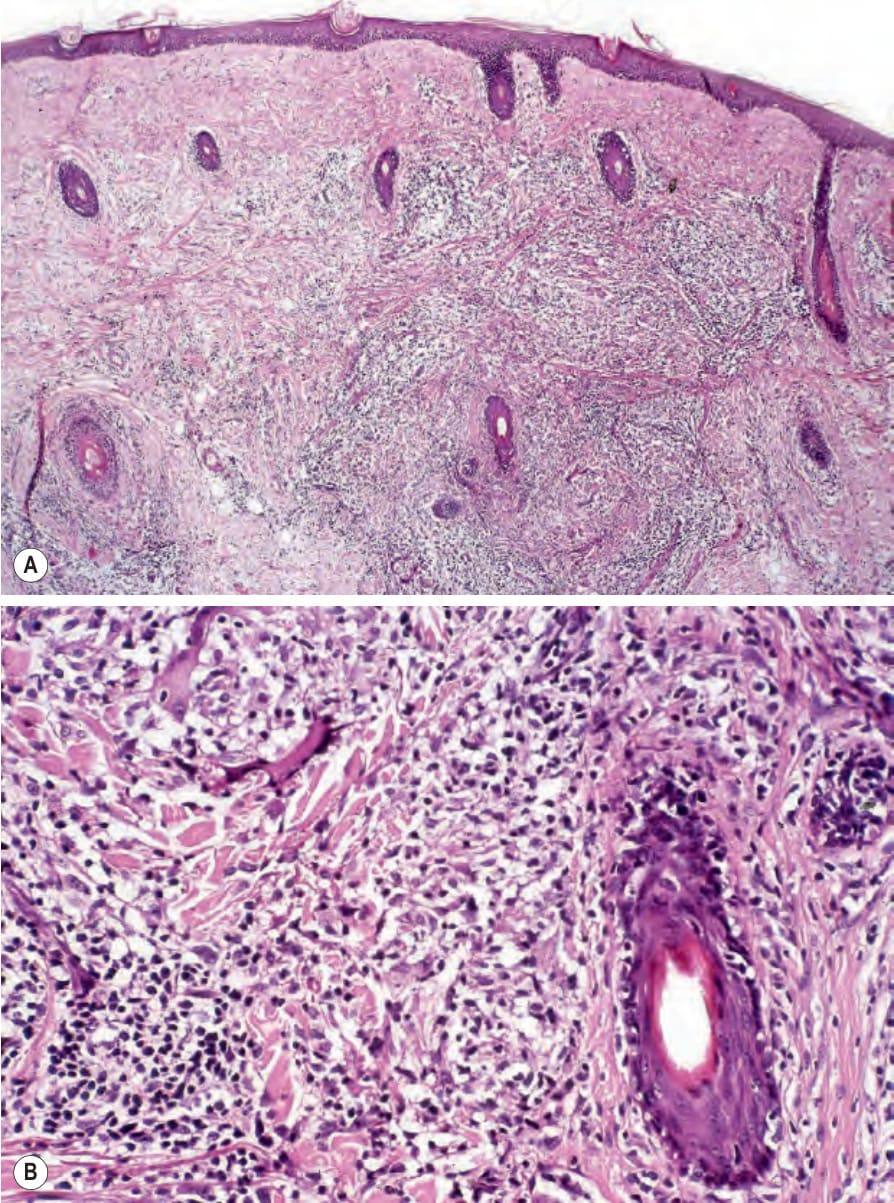
Fig. 18.170 (A, B) Lichen scrofulosorum: note the perifollicular distribution of this well-defined granulomatous infiltrate.

Fig. 18.171 BCG reaction: there is marked swelling with overlying erythema and sinus formation. Courtesy of W. Hendson, MD, Rahima Moosa Mother and Child Hospital and the University of the Witwatersrand, Johannesburg, South Africa.
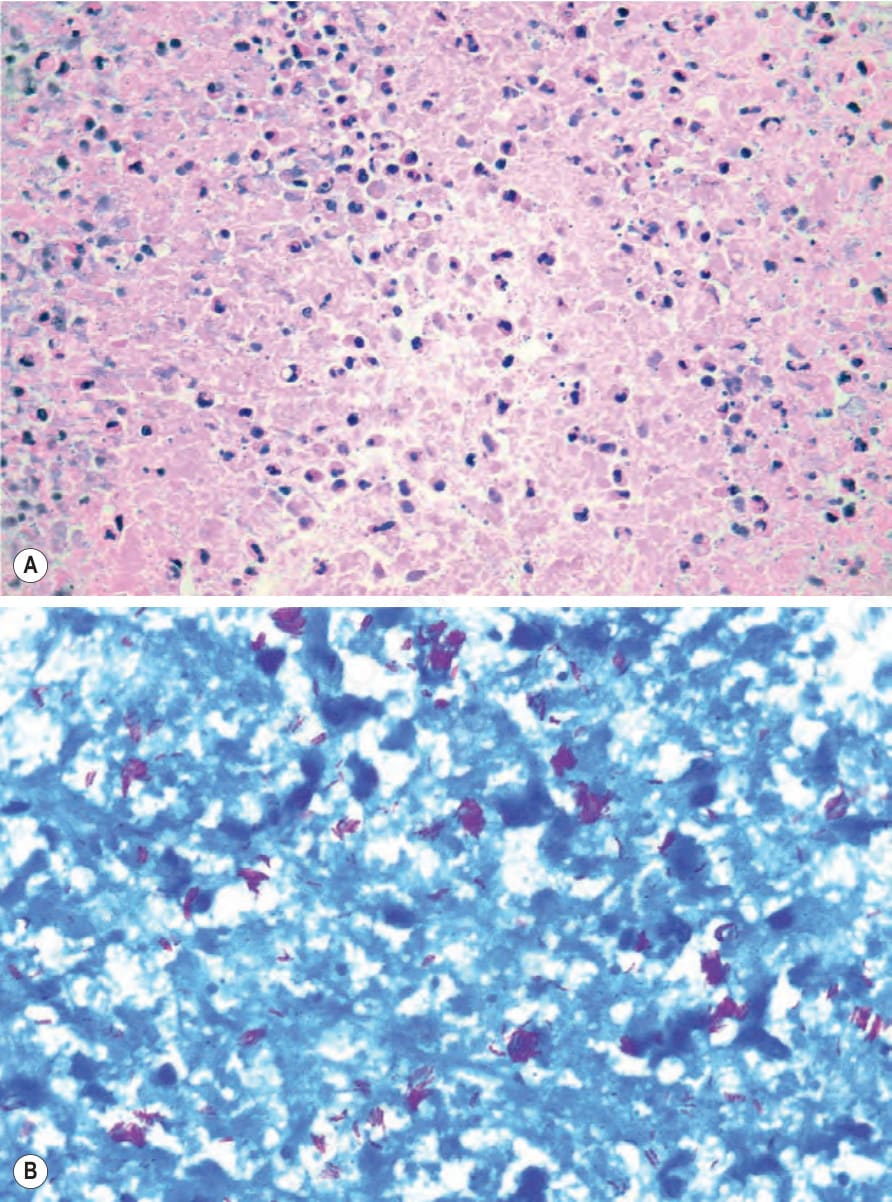
Fig. 18.172 BCG reaction: (A) there are sheet-like expanses of foamy histiocytes whose cytoplasm contains innumerable acid-fast bacilli; (B) Ziehl-Neelsen stain highlighting the latter.