Tuberculosis
Tuberculosis
Clinical features Tuberculous (Mycobacterium tuberculosis complex) infection of the skin, which was once common worldwide, had shown a declining incidence during the latter decades of the last century, especially in developed countries.1,2 This was due in part to improved therapy, a reduction in the size of the active reservoir of infection, and increased immunoresistance to infection. The late twentieth century, however, showed an apparent upward trend in the incidence of cutaneous tuberculosis, especially in Asian countries.3 A particularly important aspect of cutaneous tuberculosis is that skin lesions can readily simulate other conditions, and may be insidious in onset. The source of infection is sometimes not obvious, and tissue destruction may be very marked. Cutaneous tuberculosis accounts for 1% to 1.5% of cases of extrapulmonary tuberculosis and around 0.14% of all cases of tuberculosis.4,5
Although the global burden of tuberculosis is slowly declining, the epidemic is larger than previously estimated, and data from the WHO remain disconcerting. According to the WHO, 2015 saw an estimated 10.4 million new (incident) cases worldwide, including an estimated 480 000 cases of multidrug-resistant tuberculosis, and a further 100 000 cases of rifampicin-resistant tuberculosis. Six countries accounted for around 60% of all new infections, namely, China, India, Indonesia, Nigeria, Pakistan, and South Africa. Although the number of deaths from tuberculosis fell by 22% between 2000 and 2015, it remains one of the leading causes of death worldwide, with an estimated 1.8 million fatalities in 2015.6
incontinence are evident.1,5 A perivascular lymphocytic infiltrate is usually seen without endothelial swelling. Hyperchromic lesions exhibit epidermal atrophy, melanin incontinence, and a mild dermal lymphocytic infiltrate.1,10 Spirochetes are said to be demonstrable in all types of lesions, with the exception of late leukodermic lesions.1,11
Mycobacterial infections (tuberculous and atypical) are of increasing importance in the context of acquired immunosuppression, whether due to lymphoma, AIDS, or aggressive chemotherapy. Atypical modes of presentation with microorganisms of borderline virulence have gained significance.7 Cutaneous tuberculosis has re-emerged in those parts of the world where the incidence of HIV infection and multidrug-resistant tuberculosis is high.2,6,8,9 An estimated 1.2 million (11%) of the incident cases of tuberculosis in
881 Tuberculosis
A
and immunization programs and to an increased standard of living. Nevertheless, there remains an apparently irreducible number of people with tuberculosis, usually living in circumstances of poor hygiene and nutrition.10 This is borne out by the number of unsuspected cases of tuberculosis diagnosed at autopsy. Moreover, there exists an important reservoir of infected immigrants, particularly of Asian origin, who often present with cervical lymphadenopathy.
It is important to remember Mycobacterium bovis, the agent responsible for bovine tuberculosis, may cause zoonotic tuberculosis in humans. The estimated global prevalence of this condition in 2015 was 149 000, with the majority of infections occurring in Africa and Southeast Asia.6 Infections following BCG vaccination constitute a third form of human tuberculosis; the latter condition is discussed elsewhere in this chapter.11
The manifestations of tuberculosis in the skin are influenced by previous infection or immunity and by the route of infection. Because of the virulence and resistance to phagocytosis by M. tuberculosis, neutrophils are completely ineffective in dealing with this bacterial infection, whereas macrophages and their derivatives are characteristically seen in the cellular response. These lead on to (giant cell) granuloma formation with or without necrosis, and this underlies the varied clinical presentations of this infection.
B
2015 were HIV positive, with the vast majority occurring on the African continent, followed by Southeast Asia. The number of tuberculosis-related deaths among HIV-infected patients has declined in recent years, with around 400 000 deaths in 2015. This in part due to an increasing number of patients gaining access to ART.6
In Europe and North America, cutaneous infection is still relatively infrequent, due to a reduction in the numbers of infected cases by therapy
The majority of cases of cutaneous tuberculosis are a manifestation of systemic disease.2,8,12 The usual portals of entry of M. tuberculosis include the lungs and intestine, but the mucous membranes and skin occasionally show primary involvement.13 Cutaneous lesions include papules, nodules, plaques, ulcerative lesions, warty tumors, or scarring reactions.14 Although preferred, it is not always possible to package cutaneous tuberculous lesions neatly into the categories detailed below, and on occasion tuberculous skin disease may be reported as of non-specific type, particularly in this current era of profound immunosuppression. In this account, a modified ‘Beyt’ classification is used.2,11,15,16
Appropriate classification, when possible, is important because some variants are associated with systemic lesions and therefore clinical management and prognostic implications are highly variable.13 Tuberculids in which bacilli are not detectable are now rare in the West, but are still common in developing countries and are considered separately below.
882 Infectious diseases of the skin
Infections by inoculation (exogenous source) Tuberculous chancre, which is rare, occurs by direct inoculation of infected material into the skin of a previously uninfected and nonimmune patient.16 The response is analogous to a Ghon complex in the lung.11,15,17 These lesions develop 2–4 weeks after inoculation, which may be through minor trauma to the skin of various sites, such as the face and limbs of children (Fig. 18.146). Infection may also follow minor surgery such as ear piercing, tattooing, or circumcision. The earliest lesion is a reddish-brown papule, which may rapidly progress to an ulcer with ragged undermined edges. The margins of the lesion become indurated, and lymphadenopathy is usually noted at this stage. Satellite papules may be seen around the original lesion and this pattern of spread is termed ‘lupoid’. Inoculation tuberculosis from BCG injection is a similar phenomenon.18
Warty lupus (tuberculosis verrucosa cutis) occurs by inoculation of M. tuberculosis into the skin of individuals who have some degree of immunity or may have active infection elsewhere. It has been the most common variant in some series from Asia (Fig. 18.147).11,13,16,19,20 This lesion occurs classically as ‘prosector’s warts’ in pathologists or autopsy technicians, but may also be seen in butchers dealing with infected cattle (Fig. 18.148).15 Inoculation of the skin by infected sputum, even from the same patient, can cause a similar lesion. Children tend to be affected on the lower limbs or buttocks (Fig. 18.149).
genitalia, or anus (Fig. 18.150). Patients are usually hyperreactive to tuberculin testing. The lesions start as edematous red papules, which ulcerate and develop undermined edges. These ulcers are painful and neither progress or regress.
The lesion begins as a small indurated nodule with a keratotic warty surface at the site of inoculation and then slowly extends in a serpiginous manner, producing an irregular reddish-brown warty plaque. Although much of the lesion is firm, some softer areas may be present from which pus may exude. In some areas the lesion continues to extend, but elsewhere it may show focal involution to leave an atrophic pale scar. The warty component may persist for years, but usually resolves eventually.
Secondary tuberculosis (endogenous source) Orificial tuberculous ulcers are rare and occur in the skin or mucosa adjacent to an orifice draining an active tuberculous infection. They represent autoinoculation and are most commonly seen around the nose, mouth,
Scrofuloderma (L. scrofula, brood sow; derma, skin) is a complication of deep tuberculous infection of lymph node, bone, joint, or subcutaneous tissue (Figs 18.151–18.153). The lesion is seen as a bluish-red nodule, which ulcerates and discharges pus or necrotic material.11 Lesions are commonly seen in the neck, submandibular area, or axilla. There is associated scarring, and the combination of scarring and a chronic discharging ulcer may resemble hidradenitis suppurativa. Very rarely, scrofuloderma may arise from the lacrimal system.21
Infection by hematogenous spread Lupus vulgaris may occur following inoculation of bacteria into individuals showing some immunity (see above); more commonly, however, it represents hematogenous or lymphatic spread from a tuberculous focus, which is usually occult. Lesions occur mostly on the face (particularly around the nose), neck, and earlobes in the West, and are more common in women
883 Tuberculosis
A
B
(Figs 18.154 and 18.155).18 The extremities and buttocks are more commonly involved in patients in the East. The arms and legs may also be affected (Fig. 18.156). It is a very chronic disease. This form of cutaneous tuberculosis used to be particularly evident in Northern Europe and is still the most frequently encountered variant in the West.2,11 It is a common form of cutaneous tuberculosis in childhood.12,22
Lupus vulgaris occasionally results from direct inoculation and may even occur at the site of BCG inoculation.23
Lupus vulgaris is characterized by papules and raised erythematous and sometimes scaly plaques of gelatinous consistency, said with diascopy to resemble apple jelly. These lesions may gradually extend, while involuting with scarring in other areas. There may be adjacent cellulitis or ulceration. Extensive facial lesions can result in gross disfigurement.24,25 Squamous and
basal cell carcinoma, melanoma, and lymphoma may develop in chronic lupus vulgaris.26–29 Contractures and lymphedema are late complications. Ocular involvement is an additional serious complication. Lupus vulgaris is a rare cause of alopecia.30
Tuberculous gumma represents a metastatic tuberculous subcutaneous abscess derived from infection at another site by a hematogenous route.13,16 It is most commonly seen in the malnourished, the immunodeficient, or the immunosuppressed.8,13,31 Clinically, it presents as a firm subcutaneous nodule, usually on the arms or legs. The lesion slowly becomes fluctuant, and the overlying skin perforates to form a chronic undermined ulcer as seen in scrofuloderma.

Fig. 18.142 Late yaws: note the cyst with an overlying periosteal reaction. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
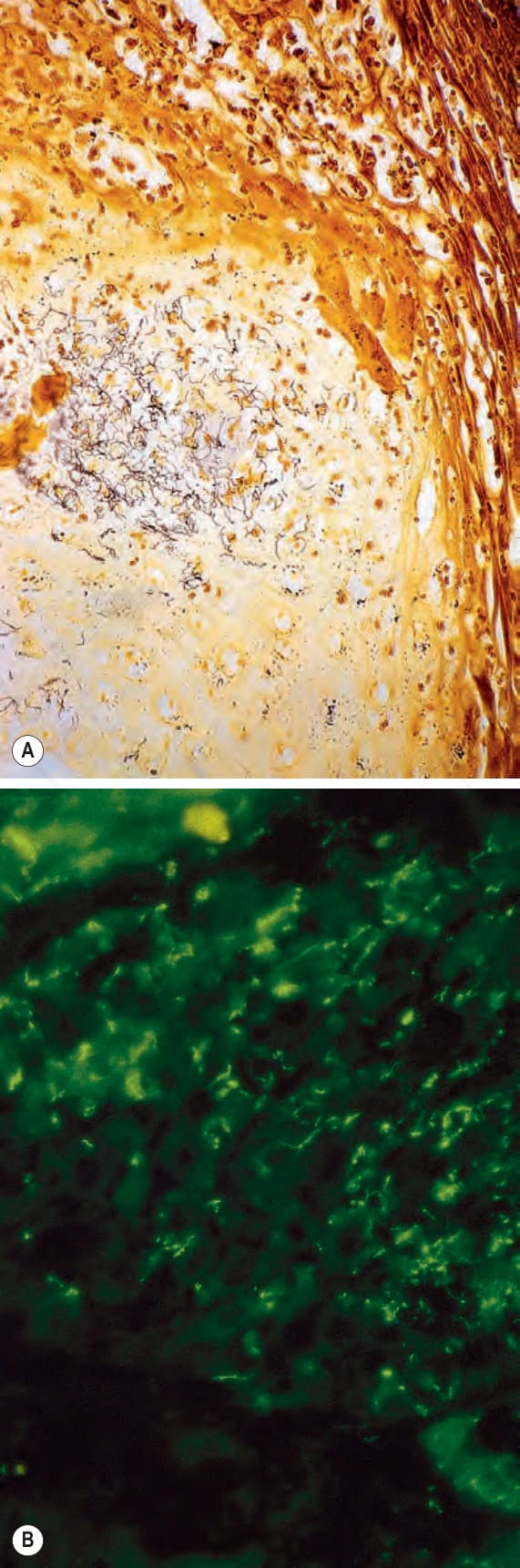
Fig. 18.144 (A, B) Early yaws: same specimen as that shown in Fig. 18.140. Note the presence of numerous spirochetes. (A) Warthin-Starry; (B) immunofluorescence. By courtesy of H.J.H. Engelkens, MD, and E. Stolz, MD, University Hospital, Rotterdam-Dijkzigt and Erasmus University, Rotterdam, The Netherlands.
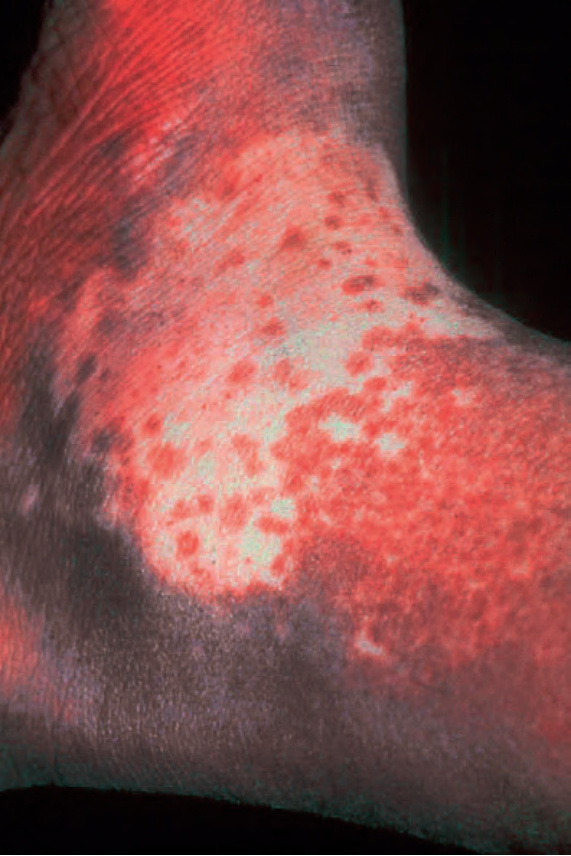
Fig. 18.145 Pinta: this is a late lesion showing characteristic complete loss of pigmentation surrounded by a hyperpigmented border. By courtesy of R. Arenas, MD, and J. Salas, MD, Azteca, Monterrey, Mexico.

Fig. 18.146 Tuberculous chancre: the cutaneous equivalent of a Ghon complex. Note the healing lesion on the outer aspect of the knee and the ulcerated inguinal nodes from this patient from the 1950s. By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.

Fig. 18.147 Warty lupus: in this example, there is a grossly hyperkeratotic lesion associated with destruction of the nail. By courtesy of the Institute of Dermatology, London, UK.

Fig. 18.148 Warty lupus: prosector’s wart. This indurated lesion on the finger developed after a pathologist had performed a tuberculous autopsy. By courtesy of R. Vellor, MD, St Thomas’ Hospital, London, UK.

Fig. 18.149 Warty lupus: in children, the buttock is a commonly affected site. By courtesy of the Institute of Dermatology, London, UK.

Fig. 18.150 Orificial tuberculosis: widespread ulcerative lesions involving the upper lip and nostril. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.

Fig. 18.151 Scrofuloderma: (A) note the marked axillary swelling and scarring with multiple sinuses; (B) in this example, there was underlying cervical tuberculous lymphadenopathy. The puckered scarring is characteristic. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 18.152 Scrofuloderma: in this case there was underlying tuberculous osteoarticular disease. By courtesy of the Institute of Dermatology, London, UK.

Fig. 18.153 Scrofuloderma: lesions in the midline of the back commonly complicate vertebral tuberculous osteomyelitis. By courtesy of the Institute of Dermatology, London, UK.

Fig. 18.154 Lupus vulgaris: the nose is a commonly affected site. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.

Fig. 18.155 Lupus vulgaris: typical plaque with golden-yellow appearance. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 18.156 Lupus vulgaris: this is a chronic lesion showing marked scaling, erythema, and induration. Squamous cell carcinoma may occasionally supervene. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
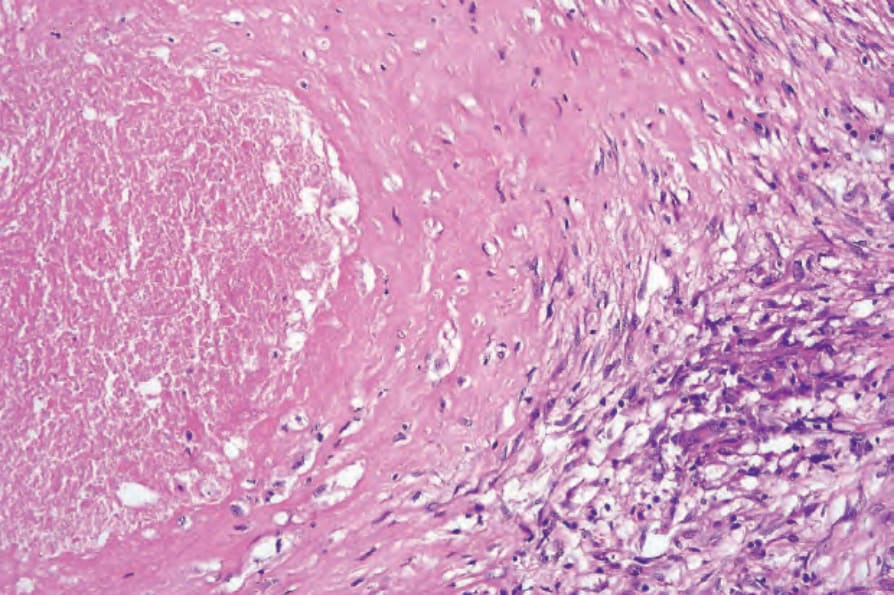
Fig. 18.159 Tuberculosis (caseation necrosis): the cell outlines are not completely lost, giving an amorphous granular appearance.
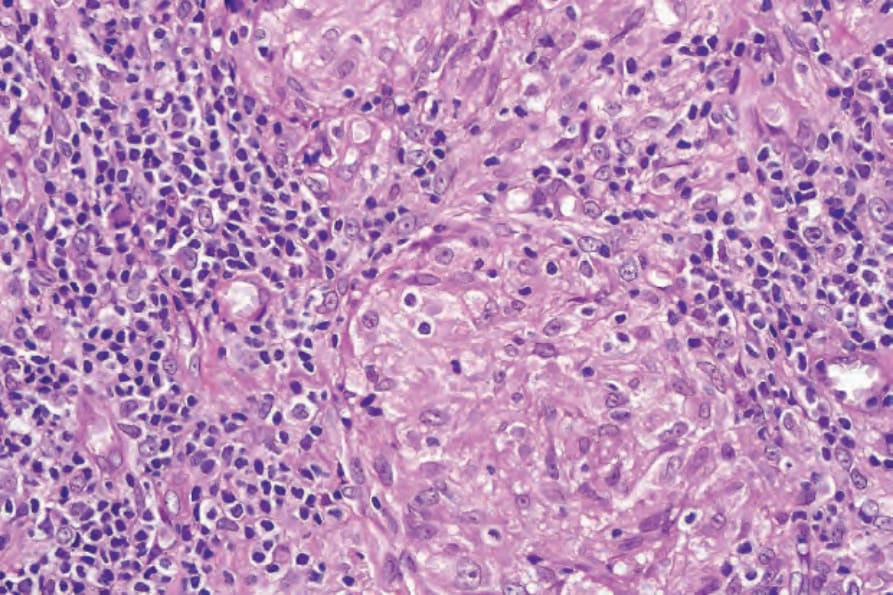
Fig. 18.163 Lupus vulgaris: the granulomata are often surrounded by lymphocytes.

Fig. 18.167 Papulonecrotic tuberculid: widely distributed small purple papules are present. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.
Miliary tuberculosis of the skin (tuberculosis cutis miliaris disseminata) occurs in association with generalized miliary tuberculosis and is very rare. It is usually seen in infants and has a poor prognosis. The infection may be seen in mother and child concurrently, and then the cutaneous lesions
884 Infectious diseases of the skin
may be scanty and the prognosis less grave.32 Other cases are associated with immunodeficiency and may follow a minor systemic infection such as measles. In these patients, there are numerous lesions which are usually centrally crusted papules or pustules, but they may be ulcerative, necrotic, hemorrhagic, or vesicular.13,16 There have been a number of reports in patients with AIDS, especially those with multidrug-resistant tuberculosis.8,9,16,33–37 The cutaneous lesions can be confused with folliculitis, resulting in delayed diagnosis.30 The prognosis is poor.8,35
Comparison of the variants of cutaneous tuberculosis is shown in Table 18.2.
Other rare manifestations of cutaneous tuberculosis that have been reported include tuberculous cellulitis, neutrophilic tuberculous panniculitis, and the presence of sporotrichoid lesions.38–43 These uncommon forms of tuberculosis have occurred in patients who were iatrogenically immunosuppressed.
Pathogenesis and histologic features M. tuberculosis, an ‘obligate pathogen’, is a slender aerobic rod, characterized by a high lipid content. This lipid is responsible for resistance to phagocytosis. It also allows the bacterium to retain basic dyes, even during treatment with strong differentiating agents, and this is the basis of the Ziehl-Neelsen/acid-fast stain (Fig. 18.157). Organisms are easily identified in tuberculous chancre, scrofuloderma, orificial lesions, and the miliary variant. They may be difficult to find or absent in lupus vulgaris, gummata, and warty tuberculosis.13 Mycobacteria are found at water-air interfaces and were so named because of their moldlike growths on the surface of liquid media.44
The organism is highly resistant to drying and therefore can retain infectivity by inoculation or contamination of minor wounds.
The reaction to the bacterium depends on:
• the size of the inoculums,
• the virulence of the organism,
• the immune state of the patient. In general, the cellular response is characterized by epithelioid macrophages, Langhans giant cells, and caseous necrosis, with lymphocytes and plasma cells in the surrounding tissue (tuberculous granuloma) (Figs 18.158 and 18.159). Tuberculoid granulomata, as seen for example in sarcoidosis, by definition do not show true caseation. The presence of large numbers of bacilli in a lesion implies a nonimmune or anergic state, such as in tuberculous chancre or orificial lesions. Caseation is an indication of hypersensitivity and is not a toxic effect of the organisms; it is clear that it is not always beneficial to the host because it is invariably associated with destruction of surrounding tissue.
885 Tuberculosis
Variant Route of infection Association with other TB Level of infection Histologic features Presence of bacilli
Tuberculous chancre Inoculation None Dermis Neutrophil abscess → caseating granuloma, lymphadenopathy
Warty lupus Inoculation Previous or current infection
Orificial ulcers Autoinoculation Active infection in associated organs
Lupus vulgaris Inoculation and/or hematogenous
Previous or current, often occult, infection
Scrofuloderma Extension from underlying infection
Present
Dermis Scanty granulomata, papillomatous acanthosis
Absent or very scanty
Submucosa dermis Mixed inflammation, few granulomata, necrosis
Numerous
Superficial dermis Variable but granulomata, little caseation prominent
May be seen in deep aspect
Active infection Subcutaneous and dermal
Mixed inflammation, granuloma, marked fibrosis
May be seen in deep aspect
Tuberculous gumma Hematogenous Systemic infection Subcutaneous Much caseation, granulomatous fibrosis
Scanty
Miliary tuberculosis Hematogenous Systemic infection Dermis Central abscess, with surrounding histiocytic infiltrate
Absent or scanty in benign form; present in aggressive form
886 Infectious diseases of the skin
Primary chancre The primary chancre is characterized by a neutrophilic abscess with numerous bacilli, associated with necrosis leading to ulceration. This is gradually surrounded by histiocytes; after 6 weeks, giant cells (derived by fusion of epithelioid cells) are seen. Central necrosis remains prominent, but diminishes, along with the number of bacilli, as the granulomatous element increases.11,13
Lupus vulgaris Lupus vulgaris is more varied in its histologic features. It is seen in the superficial dermis, consisting of tubercles, some of which coalesce, with scanty or absent central caseation surrounded by epithelioid histiocytes and multinucleate giant cells (Figs 18.162 and 18.163). Peripheral lymphocytes and plasma cells are also usually prominent. Bacteria are very infrequent. The overlying epidermis may be ulcerated (in which case there is usually a more mixed inflammatory infiltrate), atrophic, or acanthotic. The last may be severe (pseudoepitheliomatous hyperplasia), raising the problem of distinction from invasive squamous carcinoma, especially as such tumors are an important rare complication of lupus vulgaris. This may sometimes be impossible if only superficial specimens are submitted for pathological interpretation. Transepithelial elimination of granulomata has been described.45
Warty lupus Warty lupus is characterized by acanthotic papillomatosis with marked hyperkeratosis (Fig. 18.160). Pseudoepitheliomatous hyperplasia may also be seen. The dermal infiltrate consists mainly of neutrophils and lymphocytes, and abscesses may sometimes be present. Granulomata are present in the deeper dermis and caseation is occasionally a feature (Fig. 18.161).11–13 Bacilli are found on careful searching.
Orificial lesions Orificial lesions, in contrast, show extensive necrosis and numerous bacilli. The inflammatory infiltrate is not conspicuously granulomatous and may consist of lymphocytes and neutrophils, with few histiocytes.
Lupus vulgaris typically presents around the nose: this location is determined by the presence of large venous channels with stasis of blood flow and relative cold and hypoxia, which impair fibrinolysis and host defenses. Lupus vulgaris may affect other areas with relatively low temperature.
Miliary tuberculosis Miliary lesions include a severe form in which numerous central bacilli within a neutrophil abscess are surrounded by histiocytes (Fig. 18.164).
887 Tuberculosis
A
B
A
Vascular thrombi containing microorganisms may be seen.18 The less aggressive form is similar but lacks the large numbers of bacteria.
The skin lesions of disseminated miliary tuberculosis (especially in AIDS patients) are often either devoid of granulomata or exhibit only poorly formed granulomata. Extensive necrosis and abscess formation are often seen. Langhans giant cells are rare. Papillary dermal neutrophilic microabscesses reminiscent of those seen in dermatitis herpetiformis are sometimes encountered. Special stains reveal numerous acid-fast bacilli.35,37
B
Scrofuloderma Scrofuloderma usually appears as an ulcerated dermal abscess with an ill-defined histiocytic component. Peripheral granulomata may be present. Marked caseation necrosis, in which bacilli may be numerous, can be seen in the deeper tissues (Fig. 18.165).
Tuberculous gummata Subcutaneous gummata are associated with marked caseation, but there are few bacilli (Fig. 18.166). There is a surrounding granulomatous infiltrate, which may be associated with dermal involvement.
Tuberculous cellulitic lesions are characterized by granulomatous inflammation with giant cells and demonstrable bacilli.39,41,44 Panniculitis with vasculitis may occasionally be seen in cutaneous tuberculous lesions.7 Rare cases of subcutaneous mycobacterial granulomatous arteritis have been documented.46
888 Infectious diseases of the skin
Differential diagnosis The typical granulomatous and caseating picture is virtually pathognomonic for tuberculous infection, although sarcoidosis can have a similar appearance. Sarcoid, however, can be distinguished by the lack of caseation, but often this is not particularly helpful since necrosis is seen in only a minority of cases of tuberculosis. Necrosis when present in sarcoidosis is rather more fibrinoid than caseating. More helpful is the lack of a surrounding lymphocytic and plasmacytic infiltrate and fewer giant cells in sarcoidosis and a more discrete arrangement of the granulomata (the sarcoidal naked granuloma). Schaumann bodies are characteristic of sarcoidosis, but may occasionally be seen in mycobacterial infections.7
In less granulomatous forms of cutaneous tuberculosis, a distinction from leprosy must be made. The perineural distribution of the inflammation is a pointer toward leprosy.
Deep fungal infections and leishmaniasis may also be confused with tuberculosis, and recognition of the organism is vital. Granulomatous late secondary and tertiary syphilis is distinguished by the vascular changes and numerous plasma cells. Caseation necrosis is typical of acne agminata and may also be seen in foreign body reactions to beryllium and zirconium.47 It may also be a feature of Wegener granulomatosis, although this would be distinctly unusual in cutaneous lesions.
Despite these points, diagnosis may still not be possible. The difficulty is made worse by the frequent failure to demonstrate bacilli even in definite cases of tuberculosis, and the results of culture take 3–4 weeks. Therefore, occasionally, it may be a diagnosis of exclusion, which is confirmed by a therapeutic trial of antituberculous drugs.13 The shortcomings of these traditional methods have led to increased use of PCR for confirmation of the diagnosis.2,8,48
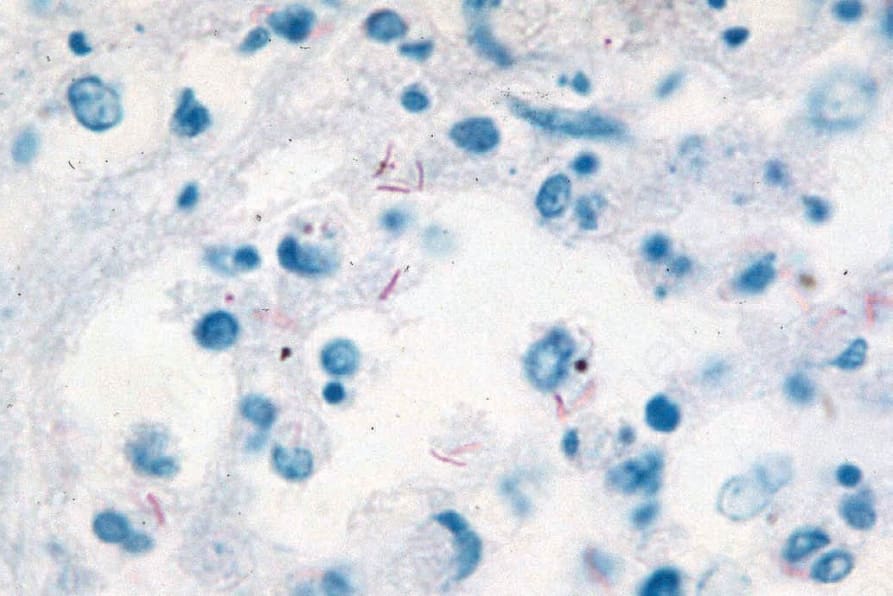
Fig. 18.157 Ziehl-Neelsen stain: in the center of the field is a small collection of red, acid-fast rods (oil immersion).
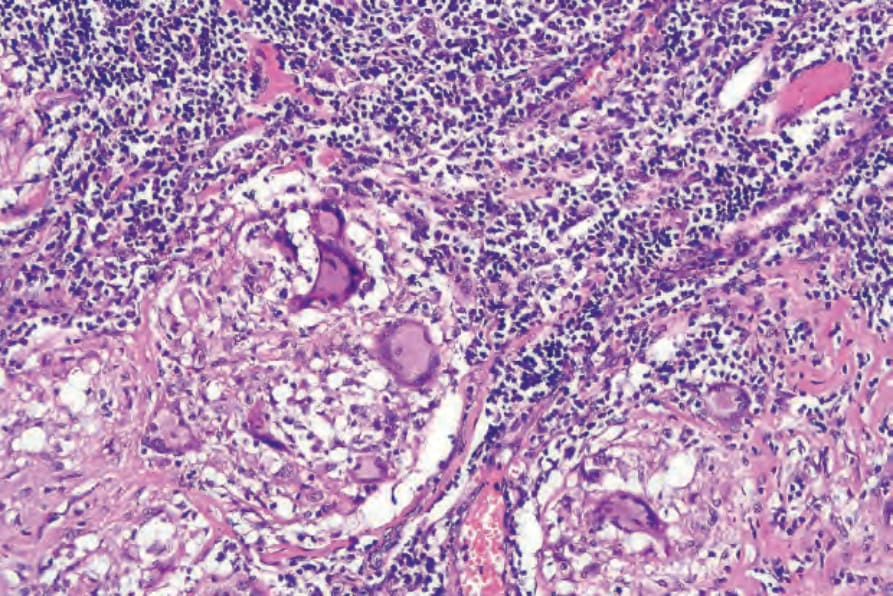
Fig. 18.158 Tuberculosis: characteristic Langhans giant cells with horseshoe peripheral rim of nuclei.
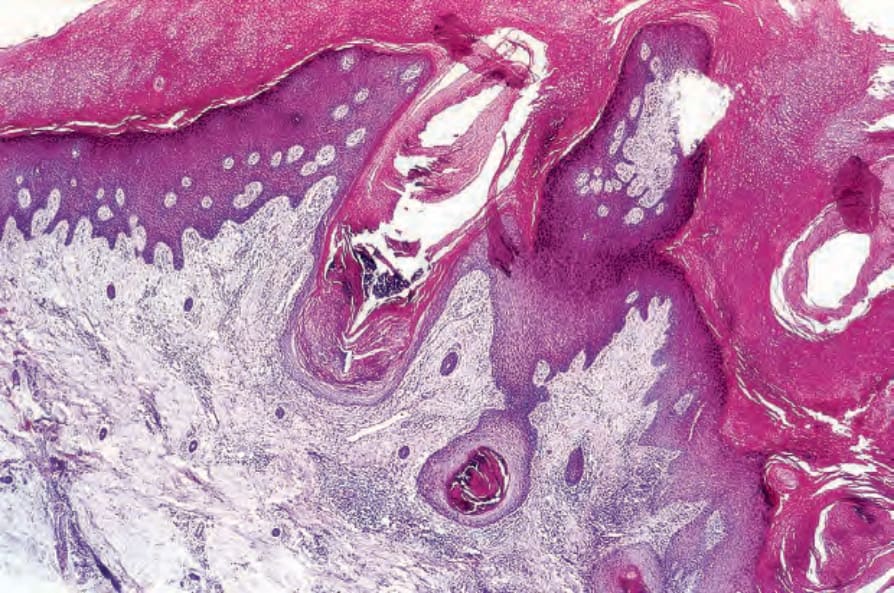
Fig. 18.160 Warty lupus: the epidermis is hyperkeratotic and shows marked irregular acanthosis. An inflammatory cell infiltrate is present in the dermis.
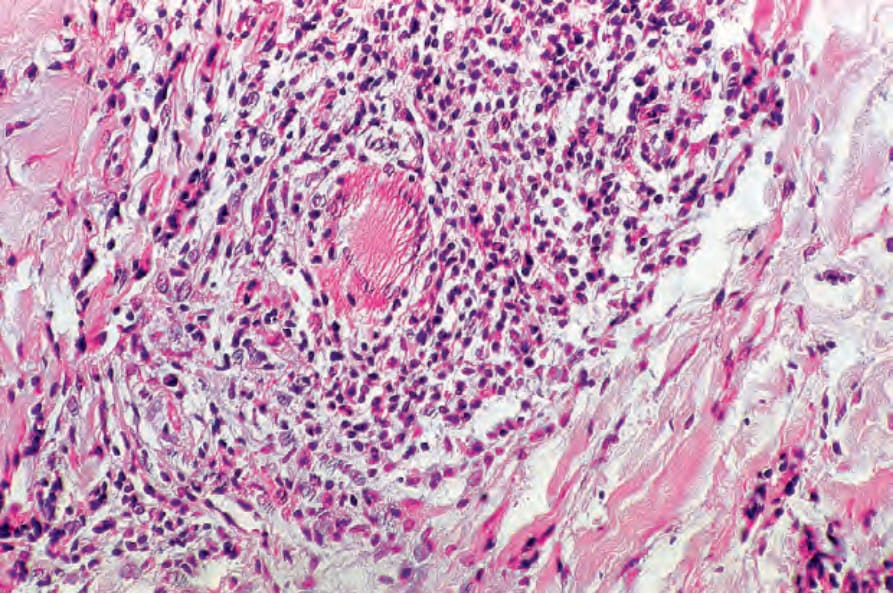
Fig. 18.161 Warty lupus: in addition to neutrophils and lymphocytes, an occasional Langhans giant cell may be present.
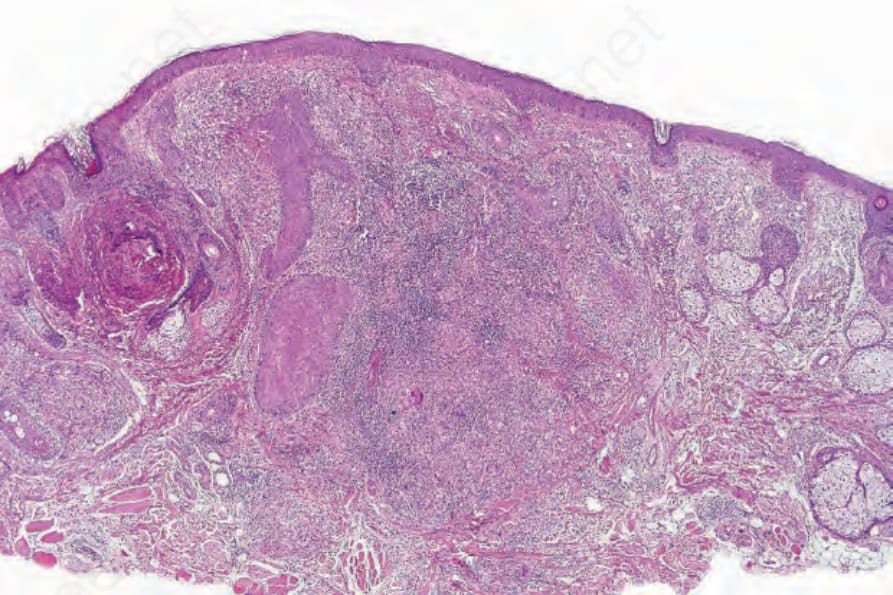
Fig. 18.162 Lupus vulgaris: there is a dense dermal infiltrate. Note the Langhans giant cell.
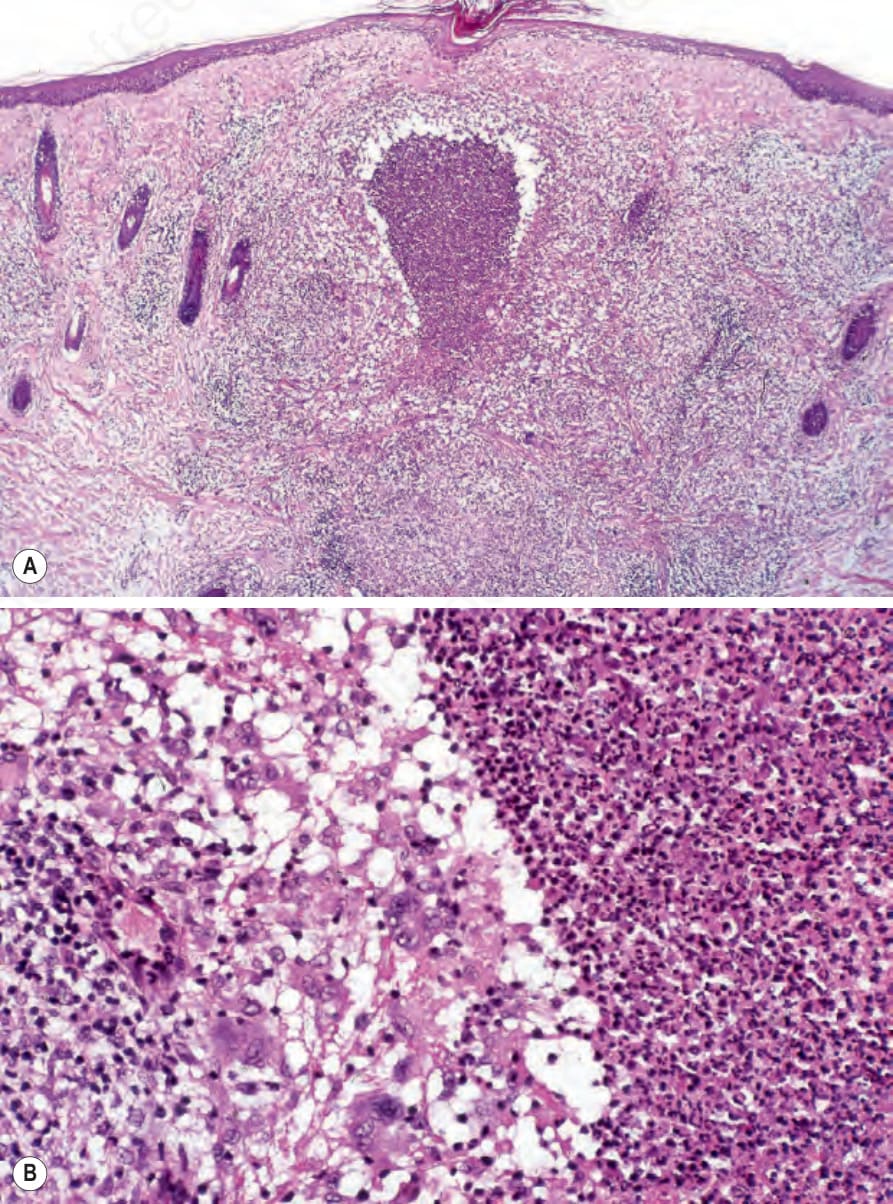
Fig. 18.164 Miliary tuberculosis: (A) a neutrophil abscess is present in the mid-dermis; (B) it is surrounded by histiocytes. Occasional giant cells are also evident.
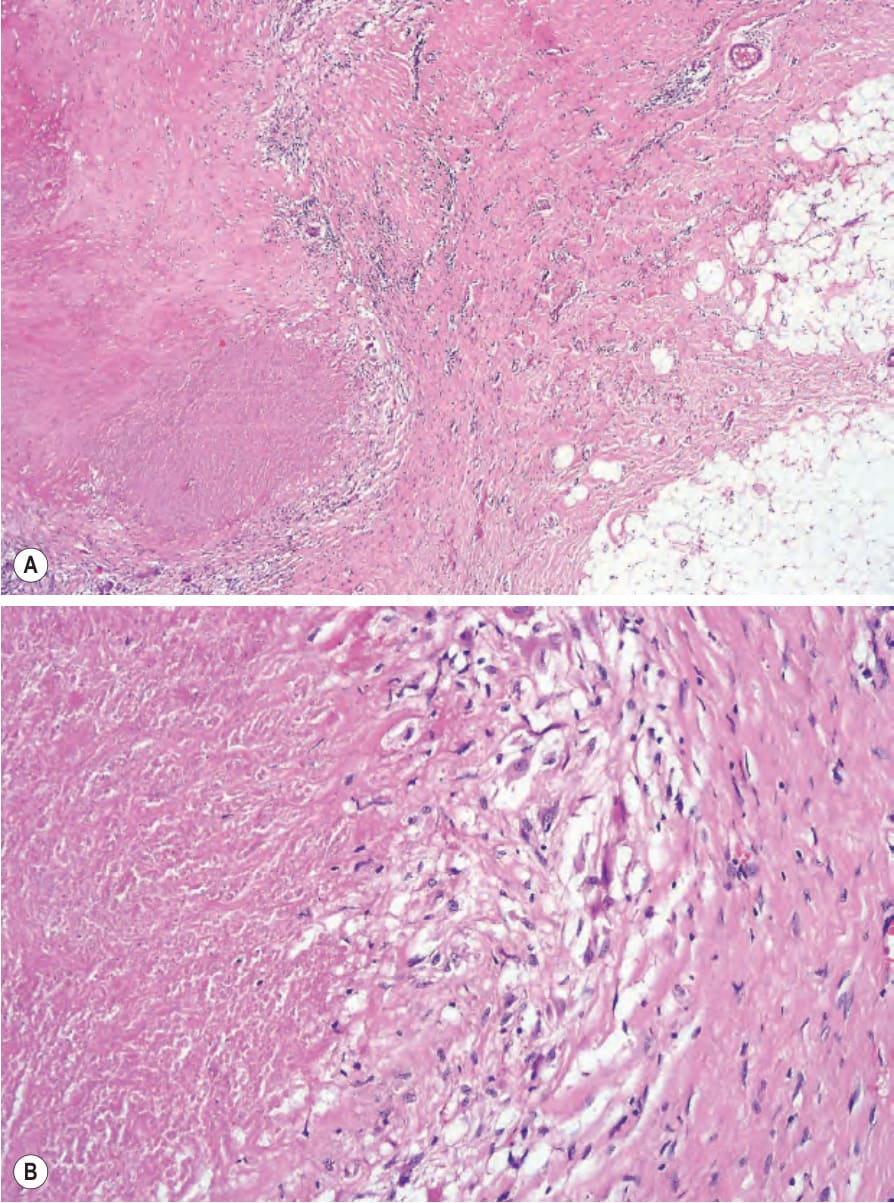
Fig. 18.165 (A, B) Scrofuloderma: there is extensive caseation necrosis.
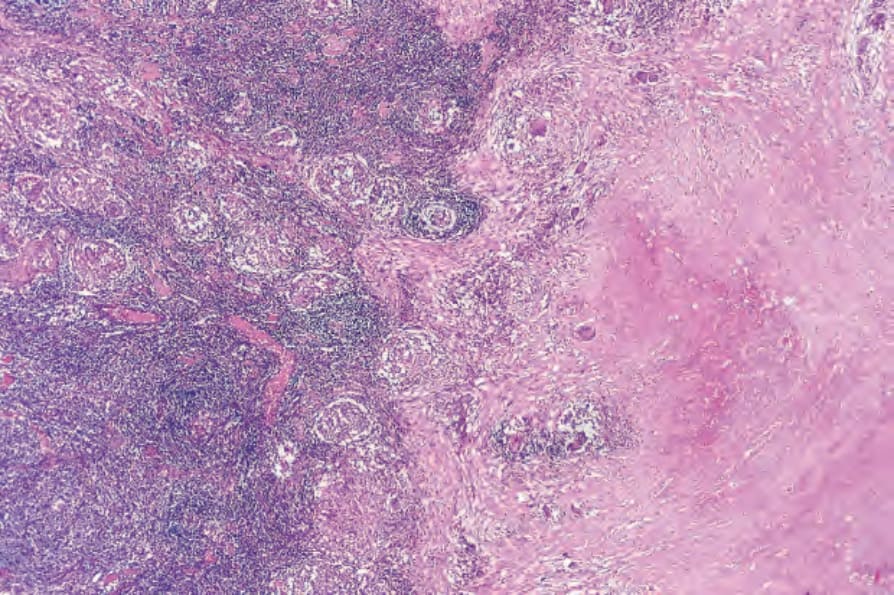
Fig. 18.166 Tuberculous gumma: there is massive caseation surrounded by a well-defined granulomatous infiltrate.
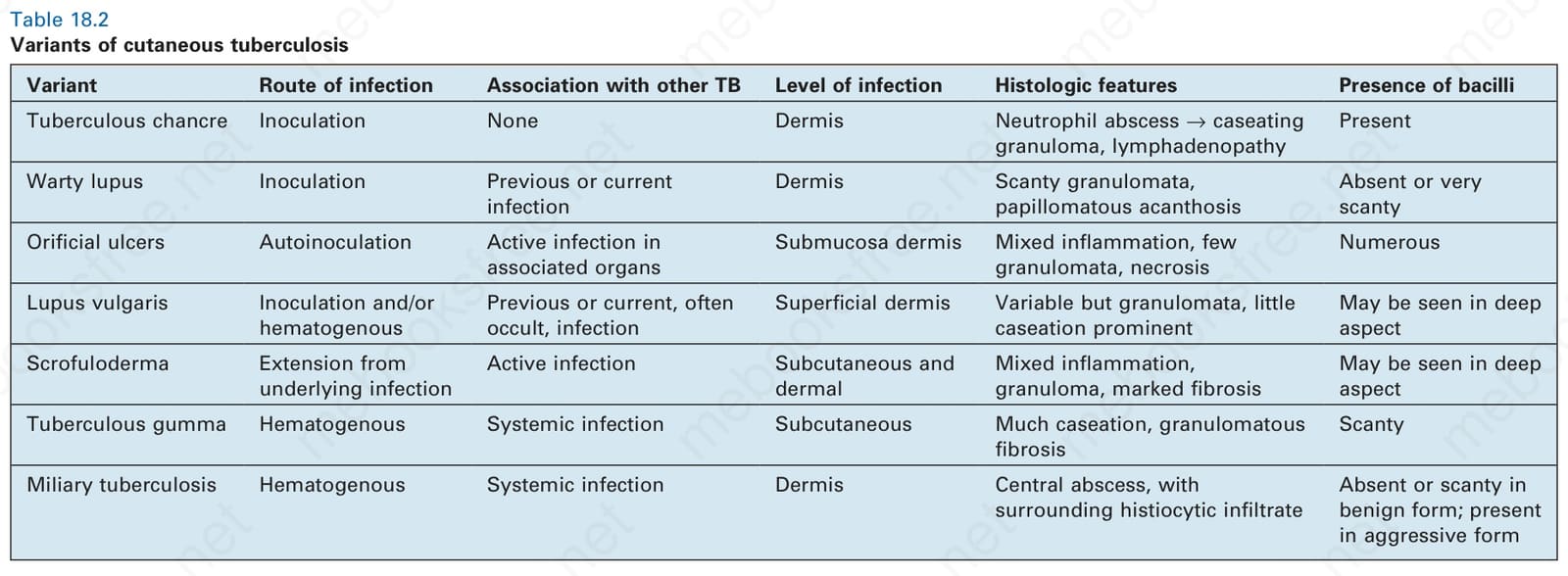
Table 18.2 Variants of cutaneous tuberculosis