Yaws
Yaws
Clinical features Yaws (framboesia tropica) is a tropical disease occurring in people living in poor conditions due to infection by the spirochete Treponema pallidum subsp. pertenue.1–6 Although the condition was thought to have been almost eradicated by the World Health Organization (WHO) mass treatment program from 1952 to 1964, which led to a 95% reduction in the global disease burden, it continues to be encountered in a number of warm, humid tropical regions including some 13 countries in Africa, Southeast Asia, and the Western Pacific region.4,7–11 In 2012, yaws was again earmarked for eradication, with 2020 set as a target date.12 Community mass treatment with azithromycin for trachoma in areas where both conditions are prevalent has had a significant impact on the number of new cases of yaws. Consequently, mass community treatment with azithromycin is a key component of the strategy to eliminate the disease.13–15 Strains of T. pallidum subsp. pertenue have been identified among nonhuman primates in parts of tropical Africa where yaws is common in humans, suggesting a possible role for an animal reservoir and cross-species infection.12,16
The triad of meningitis, cranial neuropathy, and radiculopathy has been said to be unique for Lyme disease. CNS lesions include cortical, perivascular chronic inflammatory cell infiltrates, mild spongiform changes, and gliosis. Plasma cells, however, are said to be absent. The similarity of the late CNS changes of Lyme disease and meningovascular syphilis has been stressed.32 Chronic leptomeningeal inflammation may also be evident. Peripheral nervous system lesions are characterized by nerve and ganglion lymphocyte and occasional plasma cell infiltration.17,32 Adjacent vessels may show endarteritis obliterans.
Endocardial lesions are characterized by a lymphocytic and plasma cell infiltrate; deep specimens show an interstitial myocarditis.17 Focal myonecrosis may also be evident.32
Yaws is not transmitted sexually, but rather by close contact, for example, by inoculation of skin previously traumatized by insects or scratching, and skin-to-skin contact.1,4,6,17 The disease is most common in children 6–10 years of age, who present with lesions on the feet, legs, and buttocks.1,18 Clinically, it is divided into early and late yaws.3,19–21 The initial lesion, known as a ‘mother yaw’, develops 3–5 weeks after inoculation. It starts as a nontender papilloma, which ulcerates and is then covered with a yellow crust (Fig. 18.139).3,18 It resembles a raspberry, hence the alternative designation framboesia (Dutch framboos, raspberry). This mother yaw may be surrounded by smaller papillomas, which develop 2–4 months after the initial lesion.3,6,17 Lesions in the perineum and natal cleft may become condylomatous.17 Subsequently, these warty lesions may become very widespread (‘daughter yaws’) (Fig. 18.140). Macules, papules, and nodules have also been described.18,22 They eventually resolve leaving a depressed and hyperpigmented scar.17 The mucous membranes, bones (osteitis and periostitis), and joints may also be affected in early yaws.19 Palmar and plantar hyperkeratosis, which can be exceedingly painful and may result in walking difficulties (crab yaws), are characteristic.1,22,23
Histologic examination of the synovium may show periadventitial cell onion-skinning proliferation and chronic inflammation.17,32

Fig. 18.139 Early yaws: typical framboesiform ‘mother yaw’. Note the yellow crust and surrounding hypopigmentation. By courtesy of H.J.H. Engelkens, MD, and E. Stolz, MD, University Hospital, Rotterdam-Dijkzigt and Erasmus University, Rotterdam, The Netherlands.
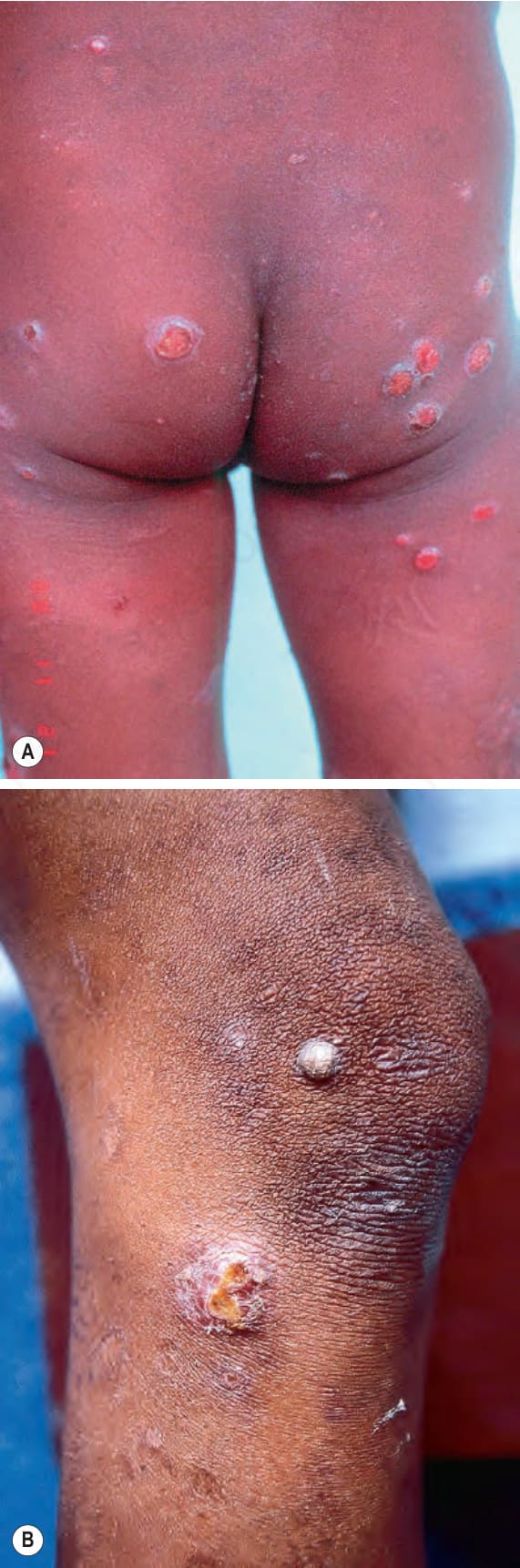
Fig. 18.140 (A, B) Early yaws: multiple smaller ‘daughter yaws’ may be widely distributed and usually present 2–4 months after the ‘mother yaw’. By courtesy of H.J.H. Engelkens, MD, and E. Stolz, MD, University Hospital, Rotterdam-Dijkzigt and Erasmus University, Rotterdam, The Netherlands.