Lyme disease
Lyme disease
Clinical features Lyme disease (Lyme borreliosis) is a generalized infection due to the spirochete Borrelia burgdorferi (B. burgdorferi sensu lato complex), of which there are three main pathogenic genospecies in humans: B. burgdorferi sensu stricto, B. garinii, and B. afzelii.1–8 Two additional species described in Europe are B. valaisiana and B. spielmanii.9 It is the most frequently diagnosed tick-borne zoonotic illness in North America and Europe.7,10 The Centers for Disease Control and Prevention (CDC) reported a 40% increase in the annual incidence of this emerging zoonosis in the United States between 2001 and 2002; more than 40 000 cases were documented during this period.11 A subsequent CDC survey revealed that more than 64 000 cases were reported in that country during the period 2003 to 2005.12 This trend has also been observed in parts of the United Kingdom and Europe.13–15 Although Lyme disease remains a relatively uncommon condition in the United Kingdom, a 3.6-fold increase in the number of annual cases was nevertheless recorded in that country in 2011 as compared with pre-2004 data.16
include granuloma annulare, papular urticaria, and Henoch-Schönlein purpura.31 Age at presentation is exceedingly variable, ranging from 15 months to 80 years. Infection rates are, however, highest among children aged 5 to 15 years, and in adults over the age of 50 years. The sex incidence is equal, and lesions present most often from May to September.10,31
Systemic symptoms (due to a spirochetemia) tend to occur early in the disease and include chills, fever, general malaise and lethargy, arthralgia, myalgia, headache, and neck stiffness. Physical examination may reveal lymphadenopathy, splenomegaly, hepatitis, and orchitis.18,32 B. garinii and B. afzelii are the pathogens most often implicated in cases of Lyme disease reported from Europe, and some authors have described differences in the clinical presentation of erythema chronicum migrans caused by these two organisms. Erythemas associated with B. garinii tend to evolve more rapidly, are often larger and homogeneous, are more often located on the trunk than the extremities, and are more frequently associated with systemic symptoms when compared with B. afzelii erythemas, which are usually annular.33,34 Patients with B. garinii infection also tend to be older, and there is a shorter incubation period.34
The disease affects most organ systems of the body.1–3 Lyme disease has been divided into three stages, I–III.17
Stage I The skin lesion of the primary stage (erythema chronicum migrans, erythema migrans) consists initially of a small erythematous papule at the site of an insect bite and expands centrifugally as a flat ring (Fig. 18.136). It is the commonest manifestation of the disease and develops on average 1–3 weeks after the bite.16,18–21 Occasionally, target lesions are described.22 Necrotic lesions are rare.23 With extension, the macules may develop a bluish or violet hue. If untreated, the ring may spread to a diameter of 50 cm before clearing. Lesional clearing is associated with a characteristic ‘bull’s-eye’ appearance. Although lesions are usually asymptomatic, patients may complain of pruritus, burning, or rarely, pain.24 The lower extremity and trunk are most often affected. Multiple lesions (usually 2 or 3) may occur.25–27 There are rare reports of vesiculobullous forms of erythema migrans.28–30
Lymphocytoma cutis (borrelial lymphocytoma), a B-cell response, may present in the acute stage and most often affects the lower ear lobes and nipples.18 It is, however, more often a feature of the third stage of the illness.19,32
Stage II Stage II disease primarily affects the cardiovascular and nervous system (meningopolyradiculitis; Garin-Bujadoux-Bannwarth syndrome).1,32,35,36 It may involve both the peripheral and central nervous systems, and tends to present 1–2 months after the primary infection; symptoms include meningism, nerve palsies (especially Bell palsy), and cerebral symptoms, including personality changes, drowsiness, or stupor.17,37 Neurological involvement is said to occur in 11% of cases.38 There have been isolated reports of orbital myositis, neurosensory hearing loss, parkinsonism, and spontaneous brain hemorrhage.39–42 Ischemic stroke may occur as a result of cerebral vasculitis.43 Cardiac involvement is encountered in 4% to 8% of patients, who may present with myocarditis and conduction defects.17,35,38,44
Approximately 50% of patients have secondary lesions, which are smaller. The palms, soles, and mucous membranes are usually unaffected.31 Erythema chronicum migrans may occasionally recur.24 Other cutaneous manifestations that have been described in the early stage of Lyme disease
Stage III Arthritis, which characterizes the third stage, presents as a recurrent, asymmetrical, and oligoarticular process involving the large joints (especially the knee) or as a migratory polyarthritis lasting up to a week in any one particular joint.32 Arthritis may occur in 45% to 60% of patients.38 Cutaneous lesions and peripheral nervous system involvement are also frequently encountered in the third stage. The typical skin lesions of late Lyme disease
are acrodermatitis chronica atrophicans, which characteristically presents as a red or violet discoloration of swollen peripheral skin, and lymphadenosis benigna cutis (borrelial lymphocytoma).19,21,24,32,45 Lesions are often bilateral. Patients may also develop sclerodermatous changes. Lichen sclerosus et atrophicus-like lesions have also been described.17,32 In the late atrophic stages of acrodermatitis chronica atrophicans, the skin may resemble crumpled tissue paper.46 Nodular or bandlike juxta-articular fibrous nodules are not uncommon, and may regress with appropriate antibiotic therapy.47 Acrodermatitis chronica atrophicans occurs mainly in Europe, where B. afzelii is the overwhelmingly predominant etiological genospecies.5,27 B. afzelii is not endemic in North America, possibly accounting for the striking geographic distribution of the condition.5
877 Lyme disease
There have been rare reports suggesting a possible association between B. burgdorferi infection and anetoderma.48,49 A case with acquired cutis laxa has also been described.50 The conflicting role of B. burgdorferi in the pathogenesis of morphea and lichen sclerosus is discussed elsewhere.51–53
Although the major clinical features are similar among European and North American cases, certain differences exist. The occurrence of acrodermatitis chronica atrophicans as an apparently European phenomenon has already been alluded to. Borrelial lymphocytoma and meningoradiculoneuritis are also observed more frequently in Europe, while multiple erythema migrans due to hematogenous dissemination in early Lyme disease is said to occur less frequently outside of North America.27 A European series of 54 cases, however, showed that 46% of patients had multiple erythema migrans lesions.25
Reinfection may occur in a small but significant proportion of patients following treatment with antibiotics. This usually manifests as a recurrent episode of erythema migrans at a different cutaneous site from the previous lesion.54,55 A Swedish study showed that women were more susceptible to reinfection than men, ascribing this phenomenon to gender differences in immune reactivity, especially in the postmenopausal age group.55
Pathogenesis and histologic features Erythema chronicum migrans was first described in association with tick bites; cases were subsequently reported following mosquito bites and thorn pricks, or without preceding trauma.44 In a proportion of cases, an encephalitis was noted and the disease was termed ‘tick-borne meningopolyneuritis’. In the 1970s, several cases were reported in the United States, and because of a clustering effect near Lyme, Connecticut, the term Lyme disease was coined (these cases had a high proportion of arthritis).38,56 The Ixodes tick has been known to be the vector for some time, but the actual etiological agent, a spirochete, was only identified in the 1980s after spirochetes were found in Ixodes dammini ticks in an endemic disease area.17,57,58 In Europe, Ixodes ricinus has been incriminated.32,44 Ixodes ticks are found widely in the temperate regions of the Northern hemisphere.10 The increased frequency of infections during the spring and summer months coincides with the time when the nymph stage of the tick is active.6
Patients recovering from the disease have been shown to have antibodies to the spirochetes in their serum.24 Spirochetes have also been identified from biopsy sites, and cultured from or detected by PCR performed on specimens of blood, cerebrospinal fluid, synovial fluid, and skin.4,21,32,44,59,60 Antibody-based tests for confirmation of the diagnosis are limited by the fact that results are more likely to be negative in the early stages of the infection.61 Immunosuppression does not appear to alter clinical presentation, treatment response, or anti-B. burgdorferi antibody production.62
Studies performed on lesional skin have revealed high levels of the T-cell-active chemokines CXCL9 and CXCL10 in erythema chronicum migrans and acrodermatitis chronica atrophicans. Borrelial lymphocytoma, on the other hand, is associated with high levels of CXCL13, a B-cell-active chemokine.69
The central component of the initial lesion shows the typical appearance of an insect bite reaction. Histology reveals a polymorphic inflammatory cell infiltrate including neutrophils, eosinophils, histiocytes, lymphocytes, and mast cells.32 Vascular proliferation and dermal necrosis may additionally be present. A superficial and deep dermal perivascular lymphocytic infiltrate characteristic of an annular erythema then develops.70 A biopsy from the periphery is non-specific, showing a perivascular and interstitial infiltrate of lymphocytes, mast cells, and plasma cells in both the superficial and deep dermis (Figs 18.137 and 18.138). Unusual histologic features, however, have been reported in some cases and present a potential diagnostic pitfall; these include spongiosis, focal interface dermatitis, an infiltrate confined to the superficial vascular plexus, and an absence of plasma cells.70
Borreliae have developed strategies to evade or inactivate host immune defenses via a variety of mechanisms.63 These include complement regulator-acquiring surface proteins (CRASPs), which confer complement resistance. Borrelial CRASPs are capable of binding FHL-1/reconectin and factor H, which are two major regulators of the alternative complement pathway.64,65 The selective up-regulation of host matrix metalloproteinase-9 by B. burgdorferi in skin lesions of erythema chronicum migrans may play a role in the local spread of the organism and its dissemination to other organs.66 In the early stage of Lyme disease, B. burgdorferi antigens induce a strong host immune response in which the production of cytokines such as IFN-γ, TNF-α, and TGF-β1 predominates.67,68 By contrast, chronic neuroborreliosis is associated with a lack of TNF-α and TGF-β1 responses.68
Identification of spirochetes by a silver stain is diagnostic.71 An immunohistochemical method for demonstrating the etiological agent has been described.32 PCR may also be used to detect the organisms in formalin-fixed, paraffin-embedded tissue specimens.72,73 One study concluded that focus floating microscopy was more sensitive than PCR in detecting Borrelia spirochetes in the lesional tissue of erythema chronicum migrans, borrelial lymphocytomas, and acrodermatitis chronica atrophicans.74 Clonal

Fig. 18.136 Lyme disease: this annular, erythematous lesion developed (several weeks later) around the site of a tick bite. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
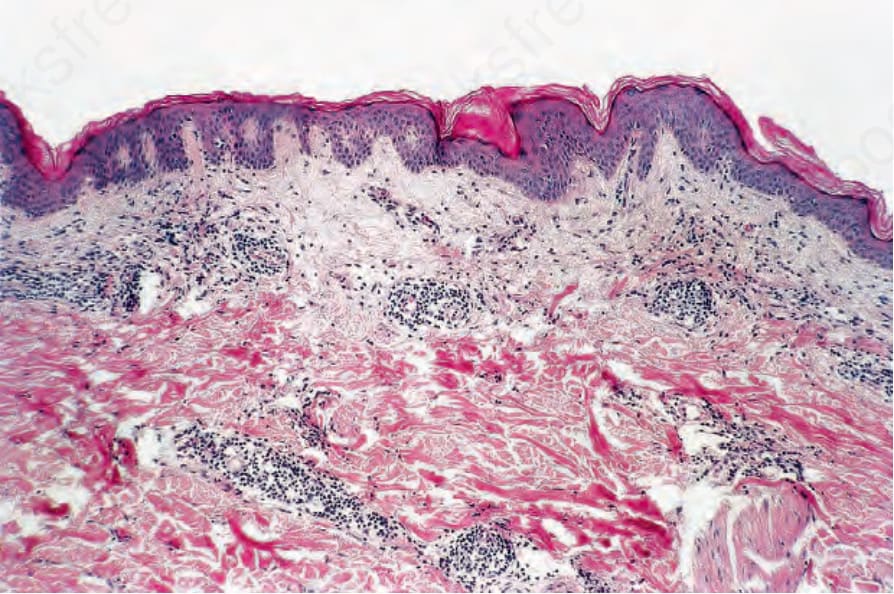
Fig. 18.137 Lyme disease: the epidermis is normal; a chronic inflammatory cell infiltrate surrounds the vessel in both the superficial and deep dermis.
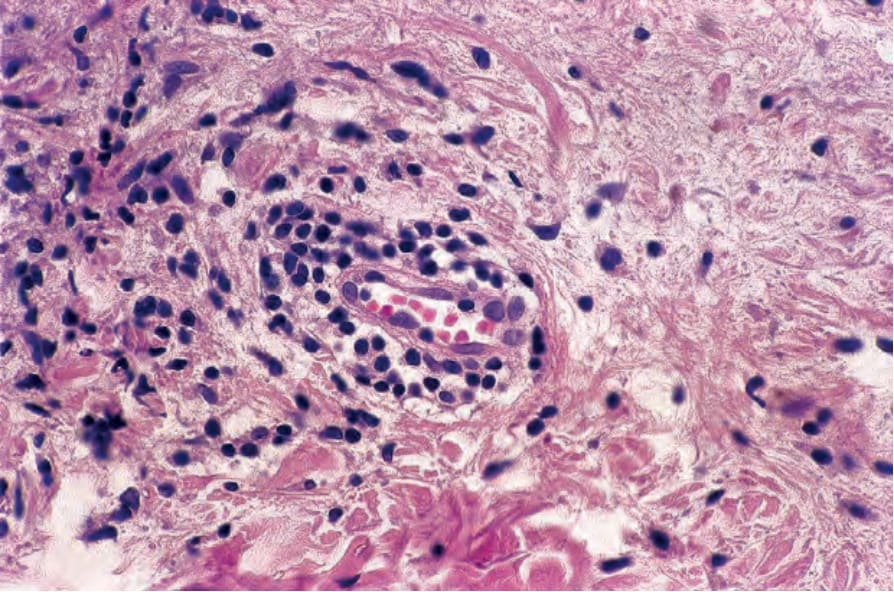
Fig. 18.138 Lyme disease: high-power view.
878 Infectious diseases of the skin
or pseudoclonal IgH gene rearrangements have been documented in DNA extracted from erythema migrans cutaneous lesions. Care should therefore be exercised when interpreting PCR results in such cases; some authors have advocated duplicate or triplicate testing.75
The borrelial lymphocytoma consists of a dense (polyclonal) dermal infiltrate composed of lymphocytes, plasma cells with macrophages, and scattered eosinophils. Although it has been suggested that germinal center formation, when present, helps to exclude a cutaneous B-cell lymphoma, this is not necessarily true; cutaneous lymphomas of marginal zone type typically display germinal centers.24,32,76 The association between B. burgdorferi infection and cutaneous B-cell lymphoma is discussed elsewhere.76,77
or joints and are clinically similar to those encountered in late yaws.1,3,9 Articular and osseous involvement is frequently destructive. Cardiovascular involvement may also occur, but the disease does not affect the CNS. A further point of distinction from venereal syphilis is the fact that there is no congenital form of endemic syphilis.1,3
Histologic features The histopathology of the primary lesion is poorly documented. The light microscopic features of the secondary lesions are virtually identical to those encountered in venereal syphilis.1,3,10 Granulomatous dermal inflammation is encountered in the tertiary skin lesions.1,10
Acrodermatitis chronica atrophicans is characterized by vascular dilatation in the mid and upper dermis accompanied by a dense infiltrate of lymphocytes, plasma cells, macrophages, and mast cells.32 Scattered groups of ‘vacuoles’ may be seen in the dermis; this phenomenon is thought to be attributable to lymphedema.46 The epidermis, which is usually hyperkeratotic, may be acanthotic or atrophic with loss of ridge pattern.17 In some patients, the appearances are reminiscent of lichen sclerosus or eosinophilic fasciitis.24,32 Occasionally, the histologic features may overlap with scleromyxedema.32 The juxta-articular fibrous nodules are characterized by fibrosis of the superficial subcutaneous tissue, with hyaline collagen bundles encircling clusters of adipocytes. There is an accompanying perivascular and interstitial inflammatory infiltrate comprising lymphocytes and plasma cells.47 Smaller periarticular fibrous nodules on the fingers show disorganized bundles of thickened dermal collagen.78