Bacillary angiomatosis
Bacillary angiomatosis
Clinical features Bacillary angiomatosis (BA) is a vasoproliferative lesion that may be readily confused with pyogenic granuloma or Kaposi sarcoma and is seen predominantly (but not exclusively) in the skin.1–4 Lesions have also been described in the bones, soft tissues, liver, lymph nodes, and spleen. Patients may have systemic manifestations including fever, malaise, hepatosplenomegaly, and lymphadenopathy.5 Although it was originally thought to be a disease specific to AIDS, it has also been described in other immunocompromised states (e.g., renal transplant recipients) and even in apparently normal individuals.2,6–13 Patients present with widespread, numerous (sometimes hundreds) of blood-red, smooth-surfaced, superficial papules and skin-colored or dusky subcutaneous nodules (Figs 18.130 and 18.131).2 The condition may be caused either by Bartonella henselae (the organism responsible for cat scratch disease) or less frequently by B. quintana (the cause of trench fever).6
A
Pathogenesis and histologic features B. henselae infection is acquired via a cat bite or scratch, or cat flea bites, whereas B. quintana infection is transmitted by body lice. Patients with BA, however, seldom seem able to corroborate this history. A PCR-based study from Johannesburg revealed a 10% rate of Bartonella bacteremia among 188 attendees at an HIV clinic, only one of whom exhibited clinical features of BA.14 Vascular endothelial cells are the prime target of the organisms following initial intracellular colonization of erythrocytes.15 The VirB type IV secretion system of Bartonella plays a crucial role in not only establishing intraerythrocytic infection but also in mediating the organism’s interaction
B
875 species Diseases caused by Bartonella species
A
B
with endothelial cells.16 Angiogenesis is potentiated by a combination of mechanisms, including inhibition of apoptosis, release of chemokines such as IL-8, and activation of hypoxia-inducible factor-1 (HIF-1).15,17–19
Histology reveals lobules of capillaries with prominent, often cuboidal vascular endothelial cells, sometimes surrounding ectatic vessels among which are dispersed neutrophil polymorphs showing leukocytoclasis and purplish granules of bacilli, which can be identified best by the Warthin-Starry reaction (Figs 18.132–18.135).4,6 Giemsa may also be used to identify the organisms, but since both the former and the latter stains are difficult to interpret and often to perform, a PCR method has been developed (see below). Sometimes solid endothelial cell proliferation is evident. Atypia and mitoses may be present.4 Superficial lesions have a polypoid configuration, and there may be an associated epidermal collarette reminiscent of a pyogenic granuloma.3,12,20 Ulceration is seen occasionally. Associated pseudoepitheliomatous epidermal hyperplasia has been described.21
Although collagen dissection by spindled endothelial cells is encountered at the periphery of some lesions, hemosiderin deposition and hyaline globules as seen in Kaposi sarcoma are not evident.20,22,23 Late, involuting lesions show extensive fibrosis of the vascularized dermis, and little by way of a polymorphonuclear leukocytic infiltrate with karyorrhexis.2,20 Such cases require a high index of suspicion, as the bacteria
876 Infectious diseases of the skin
may be difficult to demonstrate. Since most patients with this condition are immunocompromised HIV-infected individuals, it is prudent to examine sections carefully for additional opportunistic pathogens, such as CMV or mycobacteria.20,24–26
The endothelial cells can be labeled with antibodies to factor VIII-related antigen, CD31 and CD34. Histologically, liver and splenic involvement is seen as peliosis.5 Typical bacteria are, however, also present. The recognition and distinction of this infection from Kaposi sarcoma and other vasoproliferative lesions is of great importance, particularly as it readily responds to antibiotic therapy.3
Ultrastructurally, the organisms appear as aggregates of bacilli within the dermis. The bacteria have trilaminar walls.
Differential diagnosis BA must be distinguished from verruga peruana, pyogenic granuloma, epithelioid hemangioma, and Kaposi sarcoma. Pyogenic granuloma is not associated with Bartonella infection.27 The lobular capillary hemangioma (pyogenic granuloma)-like variant of Kaposi sarcoma in particular may be confused with BA.28,29 Although rare, BA with concurrent Kaposi sarcoma has been described.30 PCR or immunohistochemistry for detection of HHV-8 is a useful means of differentiating Kaposi sarcoma from BA; the former is invariably associated with HHV-8 whereas the latter has been found to be HHV-8 negative.29,31 Furthermore, PCR may be used to confirm the presence of Bartonella spp. in suspected cases of BA since these organisms are difficult to culture.32

Fig. 18.130 Bacillary angiomatosis: numerous papules and nodules are present. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.

Fig. 18.131 (A, B) Bacillary angiomatosis: the bright red coloration is characteristic. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.
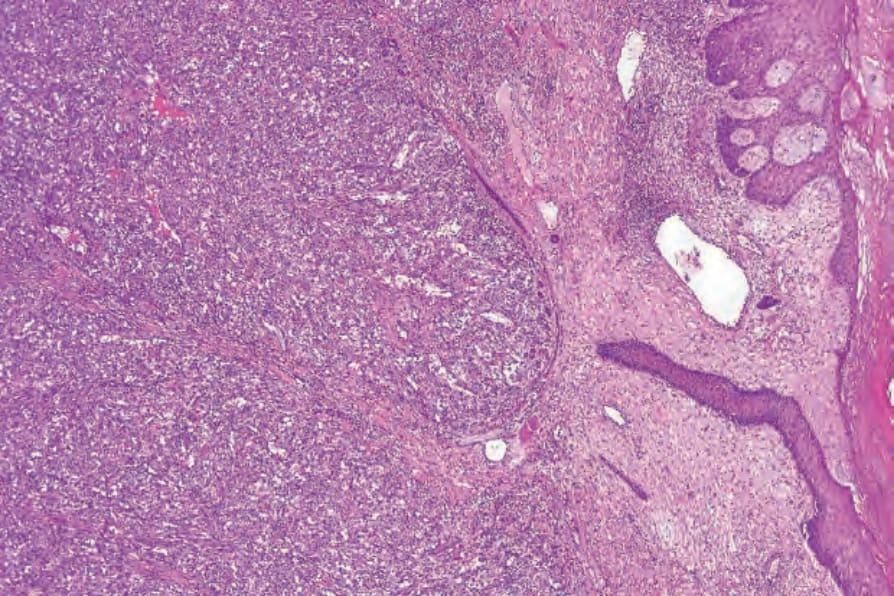
Fig. 18.132 Bacillary angiomatosis: there is a dense nodular capillary proliferative lesion; note the ectatic vessels.
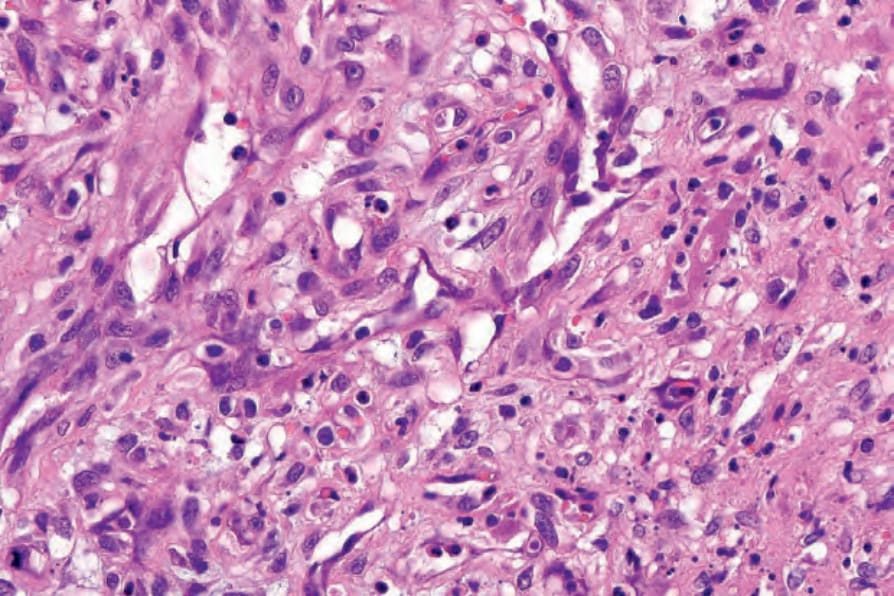
Fig. 18.133 Bacillary angiomatosis: the endothelial cells are swollen. Conspicuous neutrophils are evident.
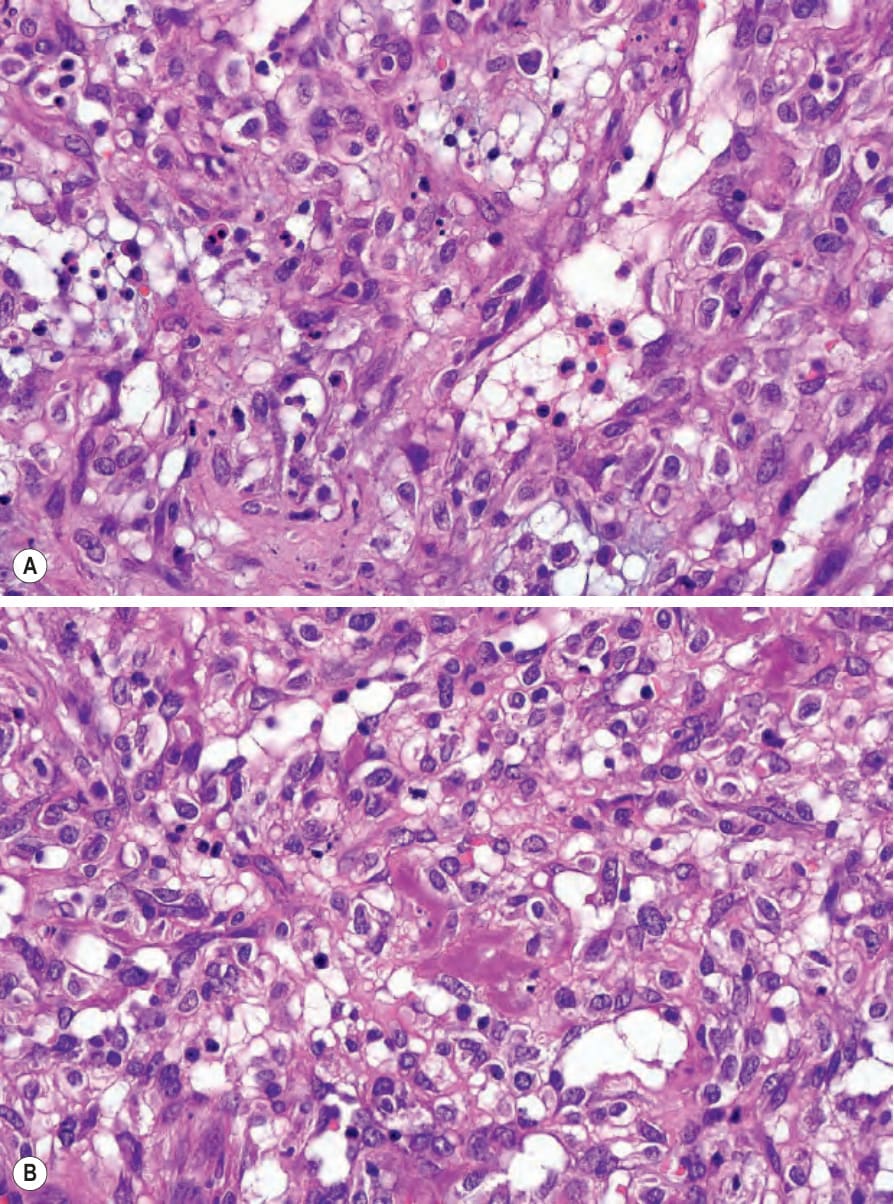
Fig. 18.134 (A, B) Bacillary angiomatosis: lymphocytes and histiocytes are also present. Note the purple colony of bacteria in the center of the field.
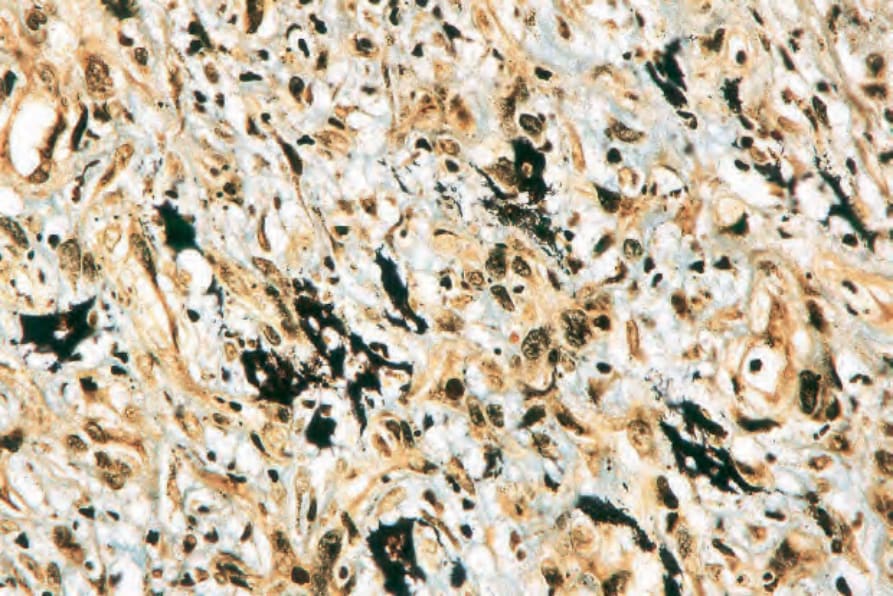
Fig. 18.135 Bacillary angiomatosis: the organisms are easily identified with the Warthin-Starry stain.

Fig. 18.136 Lyme disease: this annular, erythematous lesion developed (several weeks later) around the site of a tick bite. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.