Gonorrhea
Gonorrhea
Clinical features Plague is an acute, febrile infectious disease caused by Yersinia pestis, a nonmotile, bipolar Gram-negative aerobic bacillus and one of the most deadly pathogens known to man.1–6 Since the 1990s, the majority of human cases have been reported from Africa.7 The disease has a high incidence in Uganda, the DRC, South Africa, Madagascar, and parts of India. Foci of plague have also been reported from the United States and in parts of South America.1,2,7–11 Rodents act as the reservoir, and the infection is usually transmitted to humans via the bite of a flea; aerosol spread may also occur, leading to pneumonic plague.1,3–5 Y. pestis is well recognized as a potential bioweapon and bioterrorism agent.5,12 There are three distinct clinicopathological forms of the disease: bubonic plague, primary pneumonic plague, and primary septicemic plague.1–4,6
Clinical features This common venereal disease is due to infection with the Gram-negative intracellular diplococcus Neisseria gonorrhoeae, which especially affects the mucous membranes. In males, this results particularly in purulent urethritis, although gonococcal proctitis, epididymitis, prostatitis, and oropharyngitis may also be seen. Females most often develop endocervicitis. Urethritis and proctitis can also be features.1–3
Systemic gonococcal infection most commonly affects the skin, but may also result in arthritis and less often endocarditis or meningitis.1,3–5 Patients present with small numbers of erythematous macules that progress to painful papular, petechial, papulovesicular, or pustular lesions that particularly affect the distal limbs (Fig. 18.118).4,6,7 They measure from 1–2 mm up to 2 cm in diameter. Lesions may appear frankly vasculitic.8 Cutaneous lesions can be a presenting feature of disseminated infection during pregnancy.5,9 Rarely, however, patients present with primary cutaneous (genital and extragenital) involvement.4,6 Cellulitis, pustules, ulcers, and furuncle-like lesions
Bubonic plague Bubonic plague accounts for the vast majority of cases. After a short incubation period of approximately 2–4 days, the disease manifests abruptly with pyrexia, chills, tachycardia, and tachypnea, and the formation of a so-called bubo – a painful, pathologically enlarged unilateral group of infected lymph nodes, usually in the groin or axilla (Fig. 18.119).1 Cervical and axillary buboes are more common in children than in adults.9 Septicemia and secondary pneumonic plague may follow in untreated cases. Minor (‘ambulatory’) forms of bubonic plague also exist.1
Primary pneumonic and primary septicemic plague Primary pneumonic plague is acquired by inhalation of the organisms, whereas primary septicemic plague tends to occur after the bite of an infected flea on the head and neck region. Untreated, both of these forms of plague carry a mortality of around 90%.2
870 Infectious diseases of the skin
Cutaneous manifestations Cutaneous manifestations of Y. pestis infection are seen predominantly in bubonic plague. A small vesicle, pustule, papule, or necrotic lesion may develop at the site of the flea bite. The skin overlying the bubo is erythematous and edematous and may undergo hemorrhage and necrosis, resulting in the formation of fistulae.1,2 Roseolar, scarlatiniform, vesicopustular, and erythema multiforme-like eruptions may occur elsewhere on the body.1 Petechial hemorrhages and ecchymoses characterize severe cases. Cutaneous ulceration and necrosis may ensue, hence the term ‘black death’.2
Histologic features The lymph nodes comprising the buboes show severe acute hemorrhagic lymphadenitis in the presence of large amphophilic or ‘ground-glass’ aggregates of bacilli. Their characteristic ‘safety-pin’ appearance is discernible on sections stained with the Gramor Giemsa methods.1,2 Extranodal extension results in ulceration of the overlying skin. Subsequent septicemic illness may be complicated by DIC. In the skin, the latter manifests with intradermal hemorrhage, thrombotic vascular occlusion, and multiple cutaneous infarcts.2 The diagnosis may be confirmed by microscopy, culture, immunofluorescence, ELISA, or PCR.1–4,9 An immunohistochemical method for detection of the organism in formalin-fixed, paraffin-embedded tissue has been described.13
In its conventional form, the condition is usually acquired after contact with infected animals (herbivores) or contaminated animal products.5 It has also been described in rural Turkish children who were subjected to the ritual smearing of cow’s blood on their foreheads.17 Under ideal conditions, spores may survive in the soil or in animal products for many years.1,2 There is ongoing interest in the organism as an agent of bioterrorism.11,18,19

Fig. 18.118 Gonococcemia: pustules are commonly found on the hands and feet. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.

Fig. 18.119 Bubonic plague: note the inguinal lymphadenopathy (bubo). By courtesy of J. Frean, MD, and the late M. Isaäcson, MD, University of Witwatersrand, Johannesburg, South Africa.
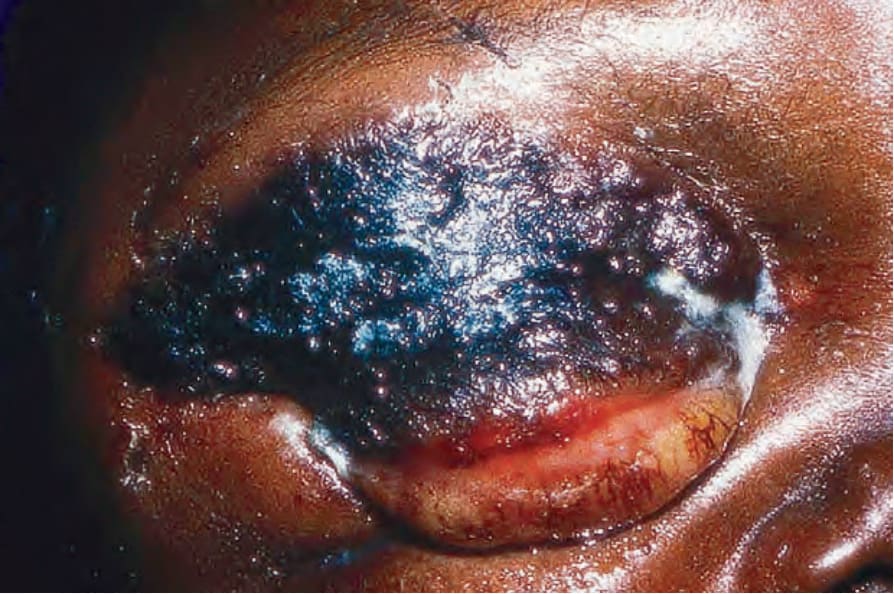
Fig. 18.120 Anthrax: cutaneous disease is the commonest manifestation in humans. This black crusted lesion is typical. By courtesy of J. Frean, MD, and the late M. Isaäcson, MD, University of Witwatersrand, Johannesburg, South Africa.

Fig. 18.121 Anthrax: multiple lesions on the forearm. By courtesy of J. Frean, MD, and the late M. Isaäcson, MD, University of Witwatersrand, Johannesburg, South Africa.