Necrotizing fasciitis
Necrotizing fasciitis
Clinical features NF is an uncommon, rapidly progressive, and potentially fatal bacterial infection of the subcutaneous soft tissues.1–6 NF may evolve following a surgical procedure (e.g., esthetic liposuction, cesarean section, laparoscopic
appendicectomy, excision of a skin lesion or even cardiac catheterization), minor trauma, seemingly insignificant scratches, in the presence of a chronic wound, or even in apparently intact skin.7–13 NF occurs predominantly in middle-aged individuals, although the pediatric population may also be affected.4,14–18 Patients with underlying diabetes mellitus, chronic alcoholism, cirrhosis, and iatrogenic immunosuppression are particularly susceptible.1,3,7,14,19–23 NF is a well-recognized complication of childhood varicella.17,18,24,25 Many reported cases have developed after intramuscular injection of non-steroidal anti-inflammatory drugs (NSAIDs), which may, in turn, mask the symptoms of evolving NF; an association with the intake of oral NSAIDs has also been documented.7,14,26–29 Rare cases have occurred following the bite of a spider.30 NF may be a rare complication of fistulating Crohn disease.31 Reported mortality ranges from 3.4% to 53%.3,5–7,14,17,25 An increased fatality rate may be encountered in the elderly and in those with worsening symptoms and signs within the first 48 hours of hospital admission.19
865 Necrotizing fasciitis
Although group A β-hemolytic streptococci (so-called ‘flesh-eating’ bacteria) were first recognized as a prime etiological agent, a number of other aerobic and even anaerobic pathogens have been implicated.4,32,33 It has become increasingly apparent that NF very often is a polymicrobial condition. In some series, Staphylococcus aureus is the most frequently cultured organism.33,34 Less often, other streptococci have been identified; these include group B and group G β-hemolytic streptococci, Streptococcus pneumoniae, anaerobic streptococci (Peptostreptococcus spp.), and S. dysgalactiae subsp. equisimilis; the latter is a recently recognized cause of NF and shares approximately 70% of its genome with group A Streptococcus, but lacks some of the virulence factors of the latter organism.27,33,35–38 Other bacteria implicated include marine organisms (Vibrio vulnificus, V. parahaemolyticus, Photobacterium damsela), members of the family Enterobacteriaceae, Serratia marcescens, Pseudomonas spp., Clostridium spp., and Bacteroides spp.15,21,33,39,40–48 There have also been isolated reports of NF due to Haemophilus influenzae serotype f, Myroides odoratus and Aeromonas sorbia.49–51 Candida albicans is an exceptionally uncommon cause of NF.52 Meleney postoperative progressive synergistic gangrene (Meleney gangrene) is synonymous with polymicrobial NF arising as a complication of surgical trauma.53 The latter condition may be clinically indistinguishable from postsurgical cutaneous amebiasis.53,54
reported mortality of this polymicrobial synergistic necrotizing infection is in the order of 16–20%, although this ranges from 3% to as high as 80% in various series.64,66,68,69,72 Extent of infection is a significant predictor of clinical outcome.72
Pathogenesis and histologic features NF due to invasive group A β-hemolytic streptococcal infection is associated predominantly with M types 1 and 3, which produce either pyrogenic exotoxin A or B, or both.32 Tissue invasion is facilitated by CD44-mediated cell signaling with subsequent manipulation of the host cytoskeleton.73,74 Superantigens and Th1 cytokines appear to play a critical role in severe group A invasive streptococcal infections.75 Streptococcal cysteine protease SpeB inactivates the antimicrobial peptide cathelicidin LL-37 at the bacterial surface.76 Impaired recruitment of polymorphonuclear leukocytes to the site of the infection has been linked to the streptococcal peptidase ScpC which degrades IL-8.77 It has been shown that a hyper-virulent phenotype ensues as a result of the organism’s destruction of its own covRS two-component system; the latter exercises a negative regulatory effect on numerous virulence factor genes.38 Protein S deficiency may be responsible for the necrosis.78 S. aureus may potentiate the β-hemolytic streptococcal infection in NF.54
The clinical presentation may be fulminant, acute, or subacute.14 NF commences as an ill-defined area of erythema, accompanied by tenderness, swelling, and increased temperature.2,55 It is, therefore, not uncommon for evolving NF to be mistaken for cellulitis or an insignificant wound infection, especially when the hallmark cutaneous necrosis is not established. This may result in a potentially life-threatening delay in diagnosis and aggressive surgical debridement, and a high index of suspicion, therefore, is required.1,2,56 The clinical features of established NF include severe pain, indurated edema, skin necrosis, cyanosis, bullae (which may be hemorrhagic, especially in cases caused by Vibrio spp.), crepitation, muscle weakness, and malodorous exudates (Fig. 18.108).1,2,23,28,42,55 Anesthesia may be a late sign.55 Patients often have other systemic manifestations of severe sepsis, including hypotension, tachycardia, tachypnea, oliguria, and mental confusion.28,57 In NF caused by streptococcal species, the latter signs are usually attributable to streptococcal toxic shock syndrome.26,58 Radiographs may reveal gas in the affected soft tissues, although this is only seen in approximately 25% of cases.2,57 NF occurs mainly on the extremities, although almost any site may be affected, including the abdominal wall, chest wall, eyelids and periorbital region, and the head and neck region.19,58,59–62 Periumbilical NF may occur in newborn infants.16,18 The Waterhouse-Friderichsen syndrome is a potential complication of NF.63
Fournier gangrene is a clinical variant of NF which involves the penis, scrotum, perineum, and abdominal wall in men and (less often) the vulva in women.64–69 An obliterative endarteritic process affecting the small branches of the superficial branch of the internal pudendal artery may play a key pathogenetic role.68,70 Because of a response to corticosteroids, Fournier gangrene may be perceived as a localized vasculitis.71 In addition to the usual risk factors such as diabetes mellitus or immunosuppression, rare associations include vasectomy or unhygienic ritual circumcision.66 Hypertension, alcoholism, and advanced age are further risk factors.69 The
An adequately sized specimen including subcutaneous soft tissue is essential for diagnosis. The histologic appearances are those of a severe necrotizing process with edema, necrosis, and inflammation involving skin and subcutaneous tissue, including fascial planes (Figs 18.109 and 18.110).79 Deep biopsies or debridement specimens containing underlying skeletal muscle may exhibit concomitant myonecrosis.4 Vascular thrombosis is encountered at all levels, and secondary vasculitic alterations are not uncommon. Hyaline necrosis of sweat glands has been described.79 The presence of large numbers of bacteria often results in diffuse basophilia of the tissue on low-power examination. A Gram or Brown-Hopps stain confirms the latter (Fig. 18.111).
Although the histologic picture is sufficiently distinctive to facilitate a diagnosis of NF, microbiological examination (including aerobic and anaerobic tissue culture) is of paramount importance in the identification of the specific infective etiological agent(s). Intraoperative frozen section has
866 Infectious diseases of the skin
a particularly useful role to play, not only in early diagnosis but also in assessing the viability of surgical margins at the time of debridement.80 PCR detection of streptococcal pyrogenic exotoxin B may be useful in confirming group A streptococcal infection when cultures are negative or unavailable.81
Differential diagnosis Necrotizing (gangrenous) cellulitis has a similar etiopathogenesis to NF but shows no extension of the necrotizing inflammatory process into subcutaneous tissue planes. This diagnosis should be made with caution and only when there is a complete absence of subcutaneous involvement in a specimen that is of sufficient depth. NF is invariably associated with necrotizing inflammation of the dermis. Furthermore, necrotizing cellulitis may be a harbinger of impending NF.
Angioinvasive deep fungal infections such as aspergillosis, hyalohyphomycosis, and mucormycosis may be associated with extensive cutaneous and subcutaneous tissue necrosis. The causative organisms in such cases, however, are often visible on careful examination of routine H&E sections, and are readily identified with the aid of appropriate histochemical stains.
A
Tissue autolysis with bacterial overgrowth may closely mimic NF, especially if tissue is obtained from a patient with a relatively minor cutaneous infection and the specimen was not placed in the appropriate formalin fixative prior to submission to the laboratory.
NF is distinguished from pyoderma gangrenosum and Sweet syndrome by the absence of true tissue necrosis and demonstrable bacterial organisms by culture or appropriate stains in the latter two conditions. Although there is frequent dermal infiltration by polymorphonuclear leukocytes in pyoderma gangrenosum and invariable neutrophilic dermatosis in Sweet syndrome, the acute inflammatory changes in both conditions are generally centered on the dermis rather than the subcutis. Vasculitic alterations may occur in both pyoderma gangrenosum and NF but are usually absent in Sweet syndrome.
B
Extravasation of anthracycline chemotherapeutic agents such as doxorubicin may be associated with extensive necrosis of skin and subcutaneous tissues, with a resultant histologic picture distinctly reminiscent of NF. The clinical history and negative Gram stain, however, argue against NF in such cases.

Fig. 18.108 Necrotizing fasciitis: this example has resulted in exposure of muscle and tendons. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
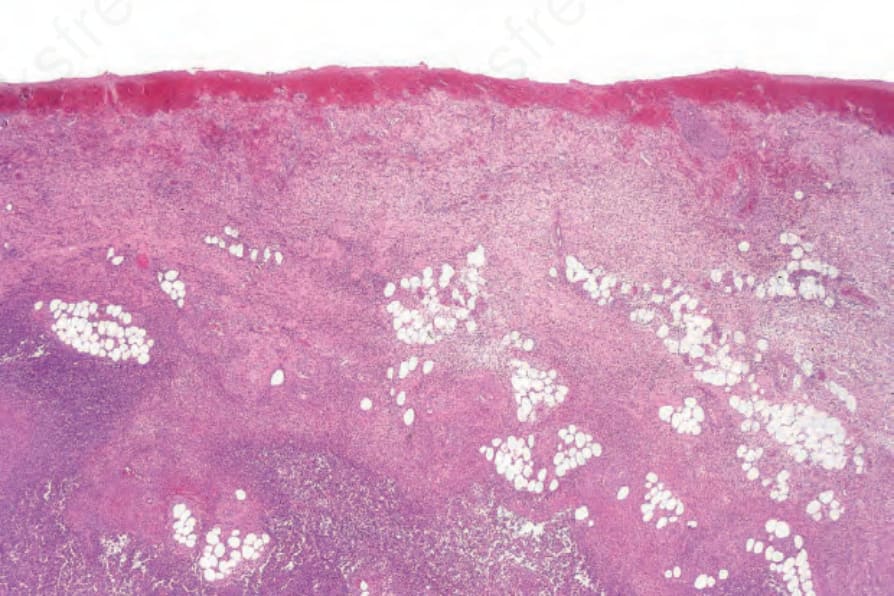
Fig. 18.109 Necrotizing fasciitis: there is intense acute inflammation of the dermis and subcutaneous fat.
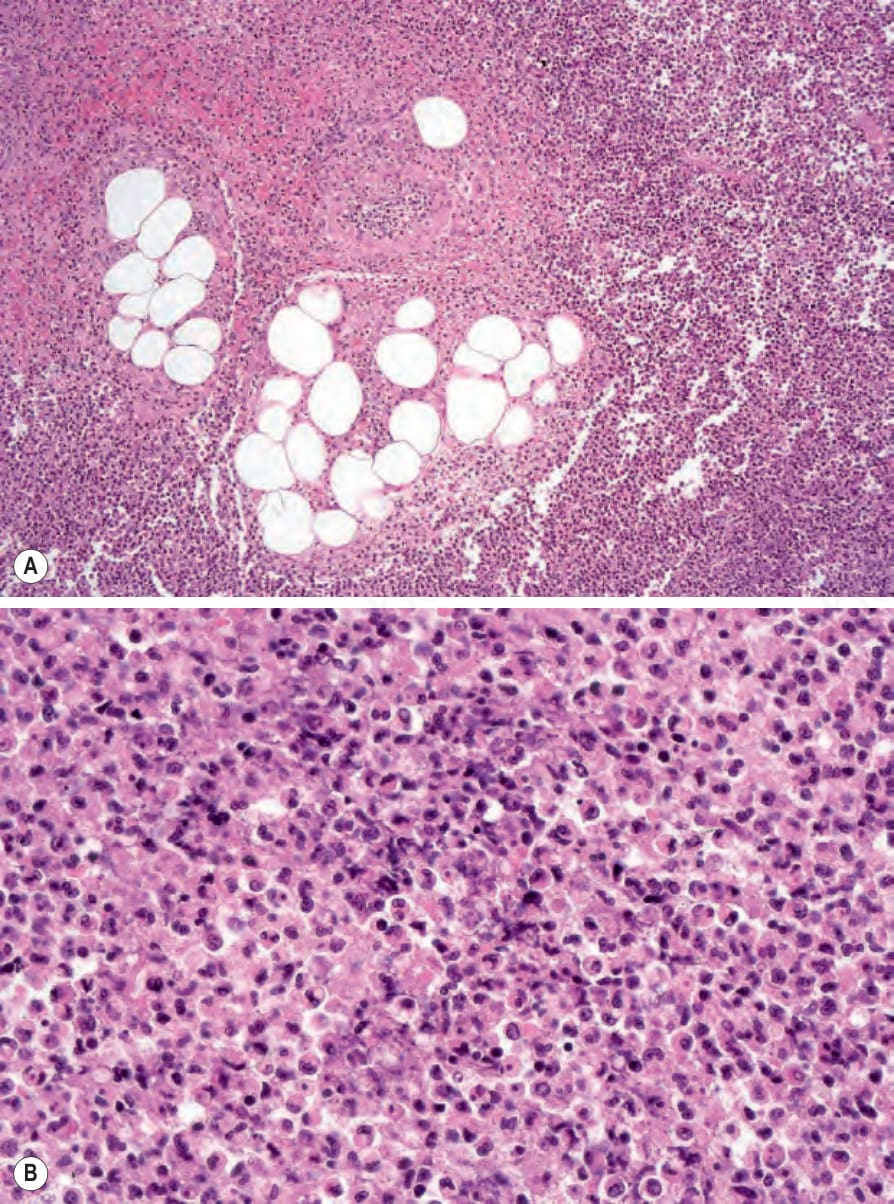
Fig. 18.110 Necrotizing fasciitis: there is an almost pure neutrophil infiltrate with necrosis.
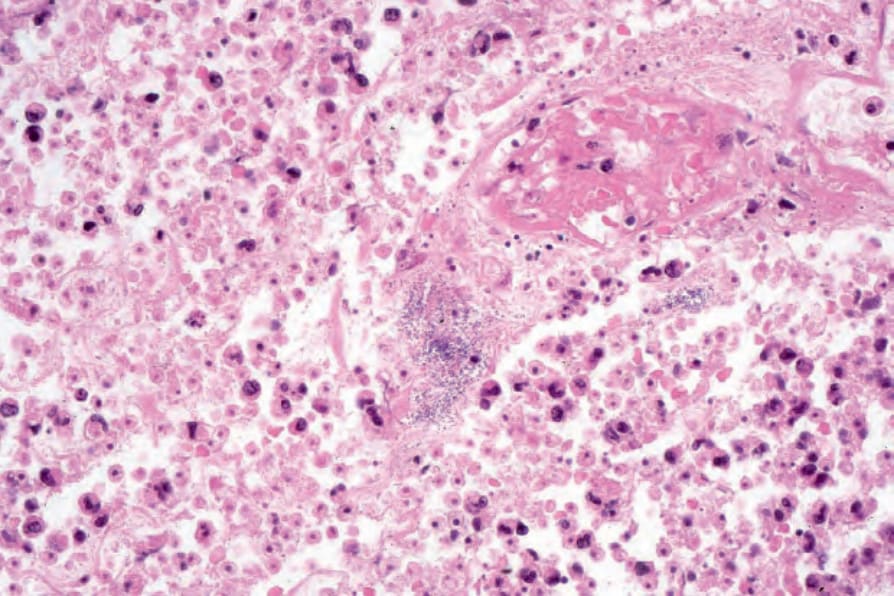
Fig. 18.111 Necrotizing fasciitis: innumerable Gram-positive cocci are present.