Trichodysplasia spinulosa
Trichodysplasia spinulosa
Trichodysplasia spinulosa (TS), also known as virus-associated trichodysplasia spinulosa, is a rare, relatively recently recognized, and novel viral infection of the hair follicle in immunocompromised patients.1–5 In 2010 it was linked to a newly discovered human polyomavirus, now termed TS-associated polyomavirus (TSPyV).4,6 The condition is mainly seen in solid organ transplant patients, particularly renal transplant, but may also occur in patients with chemotherapy-associated immunosuppression.4,6,7 It is likely that TS is the same entity as pilomatrix dysplasia and ciclosporine-induced folliculodystrophy.3,4,8,9
Clinical features TS is characterized by multiple small, skin-colored to erythematous spiky follicular papules which are asymptomatic or mildly pruritic and have predilection for the face and ears.1–5 Lesions can also occur on the trunk and limbs, although they tend to be more sparse in these locations, and may coalesce. Focal alopecia can occur. When the immunosuppression is reduced the condition improves or regresses.
Pathogenesis and histologic features TS is induced by active TSPyV infection of the hair follicle.5 Electron microscopy studies have demonstrated intranuclear viral particles of variable size, from 30 to 46 nm.1–3,7 There is clustering of infected follicular cells, which express the putative transforming TSPyV early large tumor (LT) antigen. The latter is thought to result in hyperproliferation, pRB phosphorylation, and up-regulation of p16 and p21.10
cells with eosinophilic cytoplasm and numerous trichohyaline granules are seen (Fig. 18.91). The outer root sheath persists beyond the isthmus and the bulbs are abnormal, lacking fully formed papillae. Often, there are only few matrical cells as they are replaced by large numbers of cells with eosinophilic cytoplasm. There is usually no transition between the IRS and a fully cornified hair shaft. The diagnosis may be confirmed by immunohistochemistry.11
Histologically, anagen hair follicles appear dysmorphic, with distension, dilatation, and hyperkeratosis of the infundibula and abnormal maturation with marked inner root sheath (IRS) differentiation.3,4,10 The follicles are overpopulated by IRS cells, a process has been described ‘as if the hair follicles were entirely devoted to producing inner root sheath’.2,10 Prominent
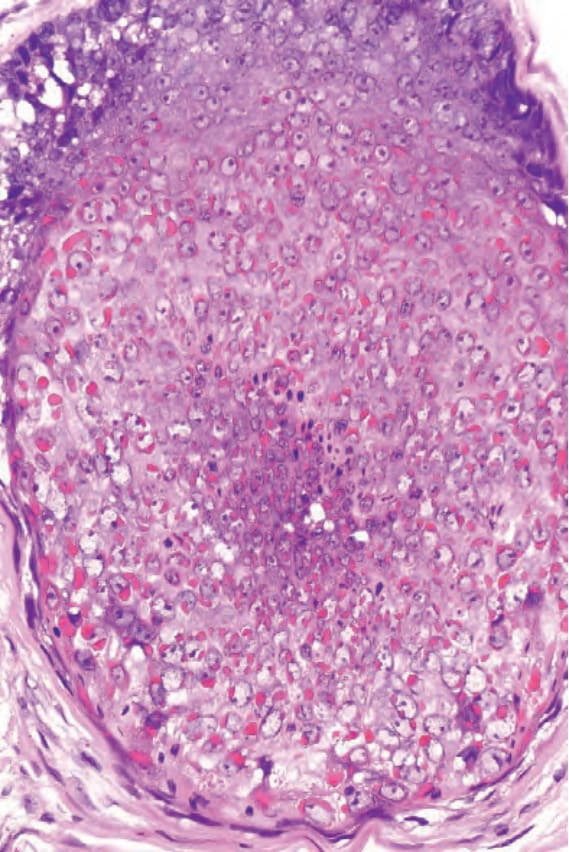
Fig. 18.91 Trichodysplasia spinulosa: note the prominent cytoplasmic granularity and eosinophilia in relation to the hair follicle epithelium.