Eruptive pseudoangiomatosis
Eruptive pseudoangiomatosis
Clinical features In 1969, Cherry et al. reported a series of four infants who developed an eruption of small hemangioma-like papules, which blanched on pressure. The lesions had an abrupt onset and apparently evolved in association with an acute echovirus infection, resolving spontaneously within a few days.1 This uncommon condition was later referred to as EPA and was initially regarded as an exanthem unique to infants and children.2,3 The more recent literature, however, reveals that more than half of all recorded cases have occurred in adults, often as small outbreaks, and especially in the Mediterranean region during the summer months.4–7 The condition is similar to or synonymous with the entity referred to in Japan as erythema punctatum Higuchi, which has been linked to mosquito bites.6,8 In children, the eruption is frequently preceded by an upper respiratory tract infection or, less commonly, gastroenteritis.3,5 Prodromal constitutional symptoms such as malaise, fever, headache, vomiting, or diarrhea are encountered more frequently in pediatric patients than in adults.5 Rare cases have occurred in iatrogenically immunosuppressed individuals.4,9,10 Isolated cases have been linked to the ingestion of a herbal medicine or food allergen.11
The acute eruption comprises numerous small, asymptomatic, bright red angiomatoid papules. The individual lesions, which measure between 2 and 5 mm in diameter, are surrounded by a distinctive pale halo and characteristically blanch on pressure.12,13 The face, trunk, and limbs are sites of predilection. Spontaneous resolution usually takes place within 3 to 10 days.3 Relapse, however, has been reported in around 70% of cases in some series.6 Exceptionally, EPA may persist for months.3
Pathogenesis and histologic features Although there is often strong circumstantial evidence to suggest that the eruption is precipitated by a viral infection, further investigation seldom leads to the identification of a specific pathogen.3,6 Isolated cases, however, have been linked to CMV infection and infection with Epstein-Barr virus.14,15 Several cases have occurred following arthropod bites, especially those of mosquitos.6,7,16 Lesions of EPA have also been induced experimentally by mosquito bites.17 Although a vector-borne infectious agent seems probable in a subset of patients, the authors of a recent meta-analysis concluded that there was insufficient epidemiological evidence to either substantiate or refute an infectious etiology.4,7 Since there is no true vascular proliferation, the authors who initially described the condition proposed that the cutaneous lesions were the result of either a direct viral effect on vascular endothelial cells or binding of antigen-antibody complexes to the endothelium.1 The latter is unlikely as there is no evidence of vasculitis. The surrounding white ring observed clinically around each lesion has been ascribed to vasoconstriction peripheral to the central zone of vasodilatation.12 It seems likely that EPA represents an unusual reaction pattern in response to a number of different viruses.2
endothelial cells into the dilated vessel lumina. Spider angiomas comprise centrally located dilated dermal arterioles with thin branches; they, too, are devoid of the prominent endothelium observed in EPA.1
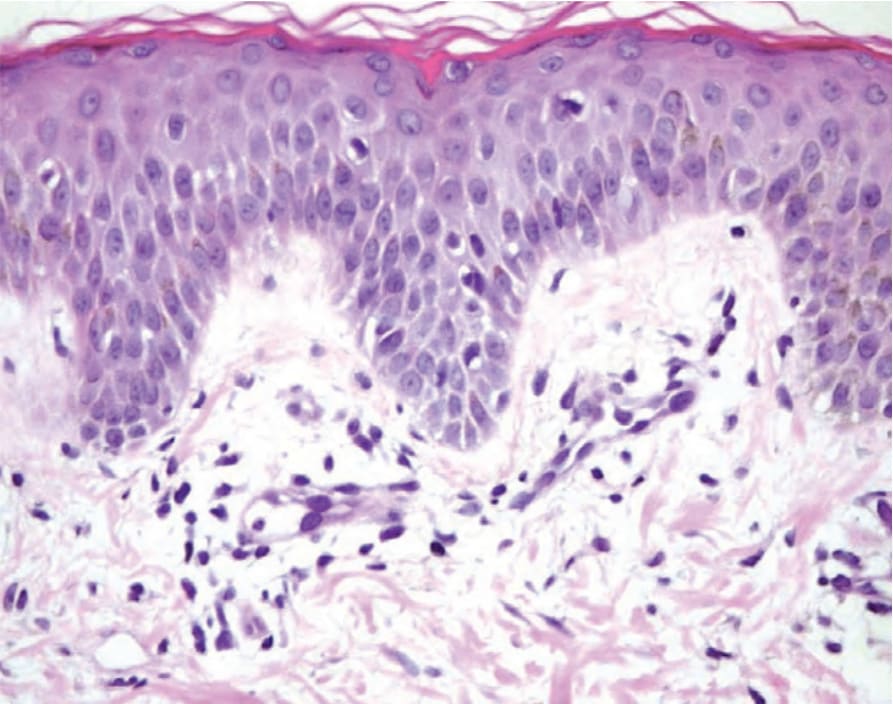
Fig. 18.62 Eruptive pseudoangiomatosis: the histologic findings are subtle, with superficial dermal vascular ectasia and relative prominence of the endothelial cells.