Measles
Measles
Clinical features Measles is a highly contagious, predominantly pediatric viral infection caused by measles virus. The latter is an enveloped, negative-sense, single-stranded virus belonging to the Morbillivirus genus in the Paramyxoviridae family.1 It is estimated that between 7 and 8 million people died annually from measles in the pre-vaccine era.2 The widespread use of vaccines against measles for more than five decades, however, led to a marked reduction in the disease.3 Recent years have nevertheless seen a resurgence of the infection, with a number of outbreaks recorded mainly in the Northern Hemisphere.4–6 Currently, an estimated 120 000 to 134 000 deaths are thought to occur annually, with some 400 measles-associated deaths worldwide per day.1,3,6 The United Kingdom saw some 477 cases of measles in the first 9 months of 2016, with 65% of the patients aged 15 years or older.6 Factors contributing to the reemergence of the disease include parental vaccine hesitancy, international travel to areas where measles is endemic, an influx of unvaccinated refugees to certain European countries, and poor vaccine coverage, with transmission between unvaccinated or incompletely immunized individuals.4–8 One of the main causes of parental vaccine hesitancy has been the unfounded suggestion of a link between autism and the administration of the MMR (measles, mumps, rubella) vaccine. Additional risk factors include immunosuppression (due to underlying HIV/AIDS, leukemia or malnutrition), and a loss of passive immunization in infants prior to an age for routine antimeasles vaccination.8
Vesiculobullous lesions are characterized by spongiosis and reticular degeneration, accompanied by epidermal multinucleate giant cells, which may contain viral inclusion bodies.26 The diagnosis of CMV infection can be confirmed by immunohistochemistry, in situ hybridization, or PCR (Fig. 18.58).69,70
Patients usually develop symptoms 7–14 days after exposure to the virus, and present initially with fever, cough, coryza, and conjunctivitis, often accompanied by malaise and a loss of appetite.6,8 An erythematous
847 Measles
maculopapular skin rash in a characteristic cephalocaudal distribution develops some 4 days later (Fig. 18.59). Patients are infective from 4 days before until 4 days after the onset of the rash.6 Whitish lesions referred to as Koplik spots appear on the buccal mucosa 2–3 days prior to the rash. The latter generally last for 3–5 days and are said to be pathognomonic of measles.6,8 The non-specific nature of the initial symptoms and the reduced incidence of the infection since the introduction of routine immunization may result in the diagnosis being overlooked. Although a majority of patients recover from the infection, a mortality rate of up to 10% has been recorded. Potential complications which may arise in the first 4–6 weeks after acute infection include viral pneumonia, secondary bacterial pneumonia, laryngotracheobronchitis, otitis media, corneal ulceration, stomatitis, and encephalitis. Subacute sclerozing panencephalitis is a much feared delayed complication of measles.3,6
Pathogenesis and histologic features Membrane fusion induced by morbillivirus glycoproteins constitutes a critical step for viral entry and replication in the host, and accounts for the predominantly lymphotropic virus’s ability to breach host epithelial barriers. Resultant syncytia formation potentiates further cell-to-cell spread of the virus. The cellular tropism of the measles virus is determined by expression of the cellular receptors CD150 and poliovirus receptor-like 4 (PVRL4) on subsets of activated immune cells (dendritic cells, macrophages, B-cells, T-cells) and on epithelial cells, respectively.1
A characteristic finding in skin biopsies is the presence of multinucleate syncytial-type epithelial cells within the epidermis and particularly hair follicles (Fig. 18.60).9–12 Apoptotic keratinocytes are not infrequently observed in the epidermis and they are quite prominent in pilosebaceous follicles, the latter being an important clue to the diagnosis (Fig. 18.61).11,12 Associated parakeratosis and a mild superficial perivascular dermal mononuclear inflammatory cell infiltrate may also be seen.9 Additional findings which have been described include intradermal syncytial giant cells, and intravascular fibrin thrombi in the presence of a mixed dermal inflammatory infiltrate harboring numerous eosinophilic leukocytes.10
Differential diagnosis Since keratinocyte apoptosis and a superficial perivascular lymphocytic infiltrate may be observed in viral exanthems other than measles, a heightened index of suspicion is required. Careful scrutiny of additional serial histologic sections, however, should enable identification of the characteristic
multinucleate epithelial giant cells encountered in measles. Although infection with HSV or VSV is frequently associated with epidermal and follicular epithelial cell multinucleation, the clinical features (including vesiculation) and presence of Cowdry-type intranuclear viral inclusions in the aforementioned herpes virus infections should readily facilitate their distinction from measles. Uncommonly, multinucleate epidermal keratinocytes may also be encountered in noninfective dermatoses, including lichen simplex chronicus, prurigo nodularis, lichen planus, and dermatitis artefacta; this phenomenon has been ascribed to chronic rubbing.13
848 Infectious diseases of the skin
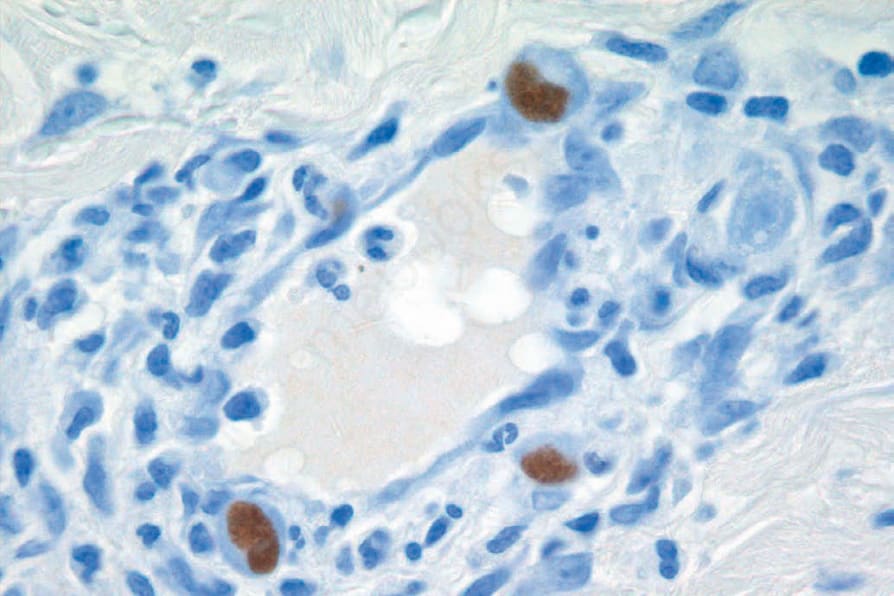
Fig. 18.58 Cytomegalovirus: positive immunohistochemistry.
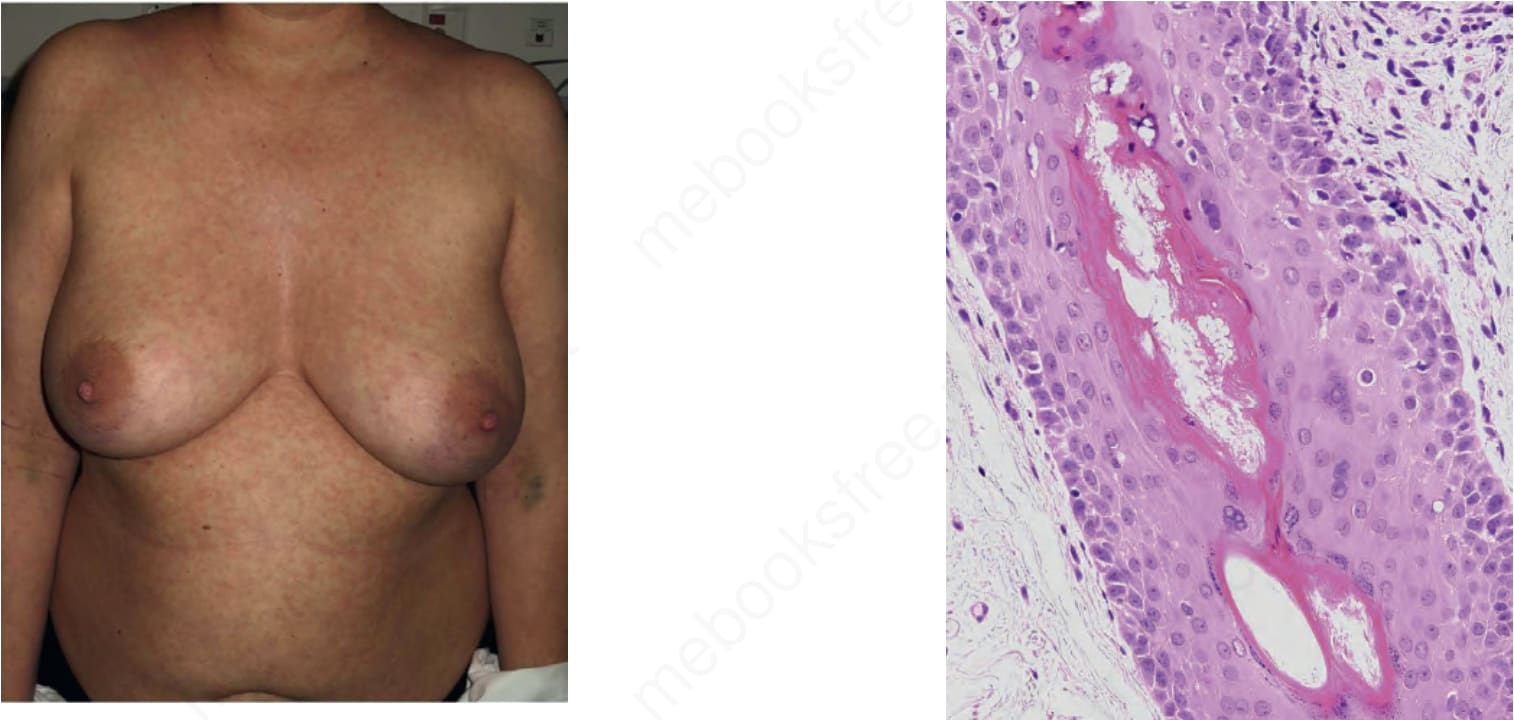
Fig. 18.59 Measles: erythematous maculopapular skin rash. The rash is usually characterized by cephalocaudal progression. By courtesy of Dr Joan Mir (Barcelona, Spain).
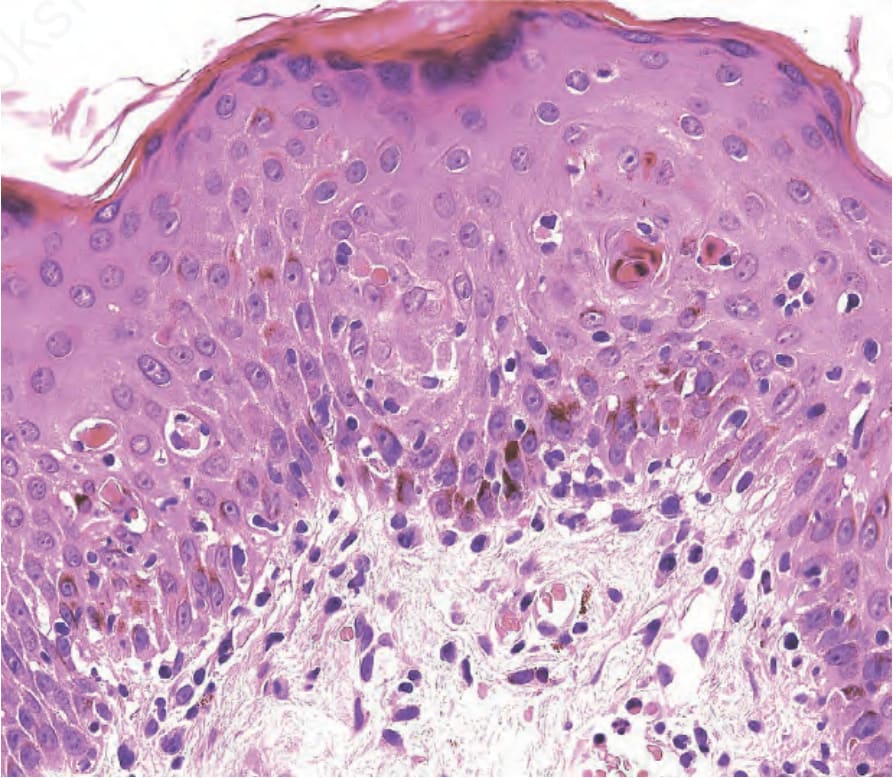
Fig. 18.61 Measles: numerous individual necrotic keratinocytes at the opening of the hair follicle into the epidermis.
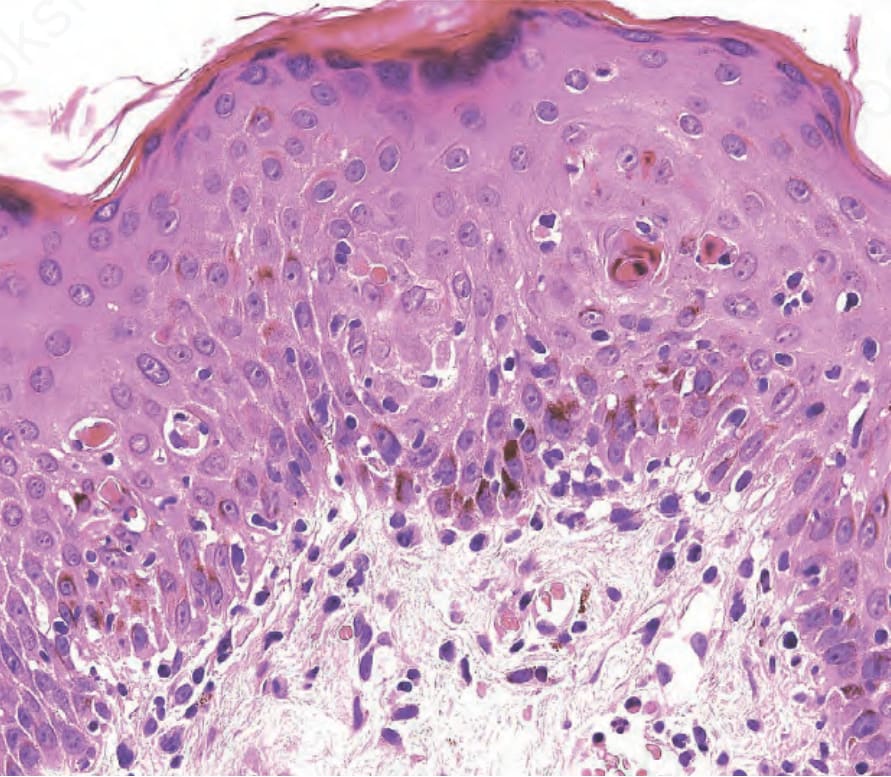
Fig. 18-60 (caption embedded in image / 圖說烘焙於圖內)