Exanthem subitum
Exanthem subitum
Clinical features Exanthem subitum (also known as roseola infantum or sixth disease) is generally a benign febrile disease of infancy and early childhood usually caused by infection with human herpesvirus 6 (HHV-6), and HHV-6B in particular.1–4 Infection with HHV-7, a closely related β-herpesvirus, however, may also manifest as exanthem subitum.4–7 Usual clinical features include high fever and a cutaneous eruption that resembles rubella or measles.5,8 Encephalitis and febrile seizures are potential complications.4,9 A case with vesicular lesions has been reported.10 Erythema and crusting at a bacille Calmette-Guérin (BCG) inoculation site has been reported in a patient with exanthem subitum.11 The diagnosis is confirmed by serology or the detection of the causative virus in body fluid or tissue samples, usually by real-time PCR.3,4
A similar exanthematous rash caused by HHV-6 infection has been reported in leukemic patients and hematopoietic stem cell transplant recipients; a possible link to GVHD has also been suggested.3,12–14 HHV-7 is also recognized as an important pathogen in transplant recipients.5,13 Other reported clinical associations and cutaneous manifestations of HHV-6 infection include papular-purpuric ‘gloves and socks’ syndrome, erythema elevatum diutinum, an infectious mononucleosis-like syndrome, Gianotti-Crosti syndrome, drug hypersensitivity syndrome, and more recently, pityriasis rosea.15–23 HHV-6 DNA has also been detected in lesions of Langerhans cell histiocytosis.24 HHV-7 has been implicated in pityriasis rosea and drug-induced hypersensitivity syndrome.23,25
Histologic features The histopathological findings in exanthem subitum are rather non-specific and include papillary dermal edema and a superficial perivascular mononuclear inflammatory cell infiltrate. Rare cases with a vesicular presentation may show mononuclear inflammatory cell exocytosis into the epidermis, with microscopic intraepidermal spongiotic vesiculation. Intranuclear inclusions (as seen in HSV infection or VZV infection) are absent. The diagnosis can be confirmed by immunofluorescence microscopy, using an antibody to HHV-6.10
The histologic hallmark is the presence of large, often purple-staining, intranuclear inclusions surrounded by a clear halo (Fig. 18.57). Smaller basophilic, periodic acid-Schiff (PAS)-positive intracytoplasmic inclusions may also be evident. These have been described within enlarged endothelial cells of dermal blood vessels, sometimes accompanied by the features of leukocytoclastic vasculitis.22,26,41,42 Inclusions may sometimes be identified in dermal fibrocytes, macrophages, and eccrine ductal epithelial cells, the last rarely associated with syringosquamous metaplasia.26,66,67 They have also been identified within the endothelial cells of blood vessels and histiocytes in the inflammatory bed deep to cutaneous ulcers (Fig. 18.57).37 Cutaneous nerve involvement (CMV neuritis) has been reported in perineal ulcers.68 In histologic specimens from immunocompromised hosts, care should be taken to rule out CMV infection in association with other infective disorders, such as HSV infection or BA.34
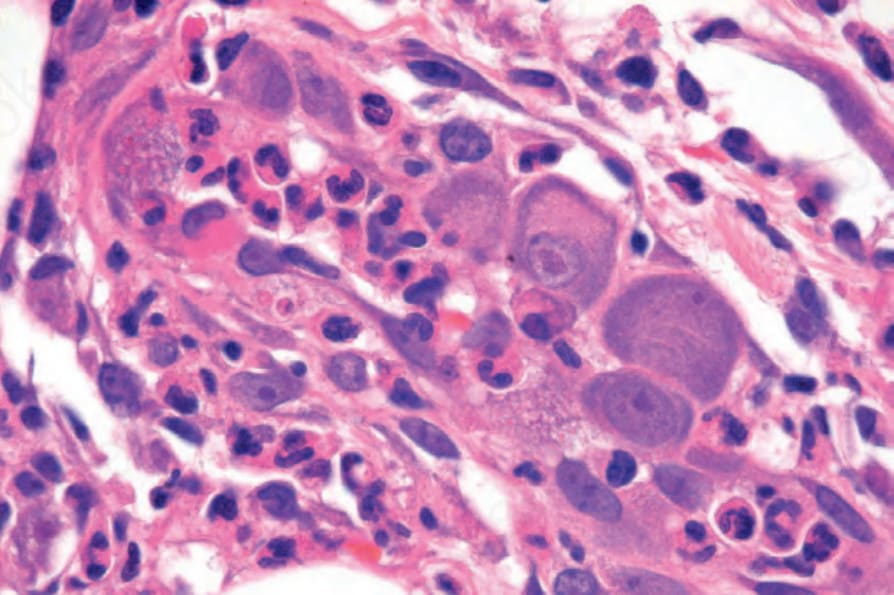
Fig. 18.57 Cytomegalovirus: high-power view showing the typical eosinophilic intranuclear inclusions.
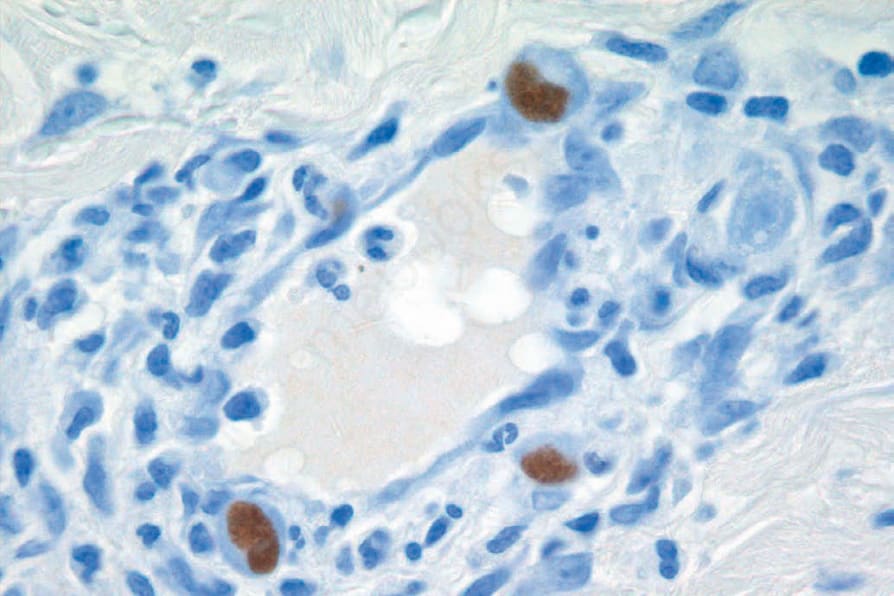
Fig. 18.58 Cytomegalovirus: positive immunohistochemistry.