Echinococcosis
Echinococcosis
Clinical features Echinococcosis is a zoonotic disease caused by a helminth, mainly the tapeworm Echinoccocus granulosus (the cause of cystic echinococcosis) but also
975 Echinococcosis
by E. multilocularis, E. vogeli, and E. oligarthus. The parasite belongs to the class Cestoda, family Taeniidae, and genus Echinococcus. It is a very important cause of morbidity not only in many developing countries but also in New Zealand and Australia. The adult worms, which measure 3–6 mm in length, reside in the small bowel of their dog, sheep, or even human host. Eggs released from the gravid proglottids into the feces are ingested by the intermediate host (man), whereupon they evolve into larvae (onchospheres) which penetrate the walls of mesenteric blood vessels in the small intestine. Most affected individuals present with disease in the liver and lungs. Subcutaneous or skin lesions are rare, occurring in only 2% of cases.1–7 The mechanism of cutaneous dissemination is the result of vascular spread, lymphatic drainage from the diaphragm, or contiguous spread when visceral lesions rupture and form cutaneous fistulae. Individuals with subcutaneous intact lesions present with an asymptomatic mass which is clinically diagnosed as a cyst. Around 90% of reported cases have been in patients from rural areas.7 The lower extremity is involved in almost 61% of cases, with the thigh being the most frequent anatomic location (27–34.8%), followed by the gluteal region (9%) and the upper extremity (8.7%).8,9 Other rarely reported sites include the subcutaneous tissues of the neck, and the thoracic spinal area.10,11 Recorded diameters range from 2 to 15 cm, with a mean of around 5.7 cm.8 Patients with fistular disease present with inflamed lesions that often develop secondary infection.
Histologic features In many cases, the cysts are intact and recognition of the parasite is not difficult. Cystic echinococcosis consists of three layers as follows:
• An outer host layer also known as the pericyst,
• A middle laminated membrane which is quite characteristic, is acellular, measures 2 mm in thickness, and allows the passage of nutrients,
• The transparent inner germinal layer which is very thin. Multiple scolices develop from the brood capsule. In a number of cases there is only a subcutaneous, palisading granulomatous reaction containing what appears to be fragments of keratin. This leads to the erroneous diagnosis of a ruptured epidermoid cyst. However, these fragments represent PAS-positive remnants of the membranes of E. granulosus mimicking keratin. Distinction is crucial as the identification of the subcutaneous parasite may lead to the diagnosis of latent visceral disease.7 It is not clear how these fragments reach the subcutaneous tissue. They may be the result of a pre-existing intact subcutaneous cyst or, based on the sparsity of the material found, they may represent circulatory spread from visceral lesions that are deposited in the subcutaneous tissue.
Access ExpertConsult.com for the complete list of references
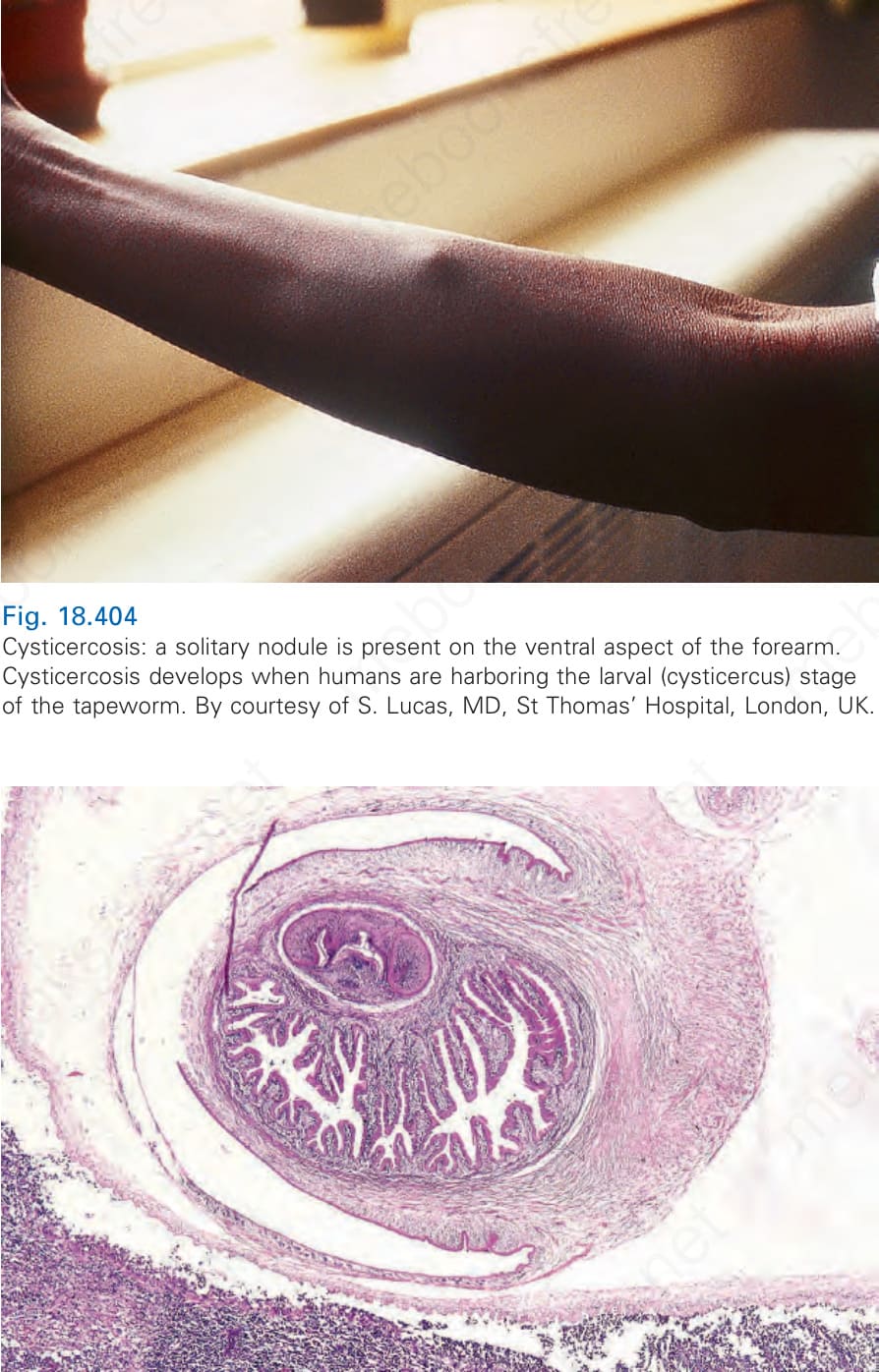
Fig. 18.404 Cysticercosis: a solitary nodule is present on the ventral aspect of the forearm. Cysticercosis develops when humans are harboring the larval (cysticercus) stage of the tapeworm. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.