Cysticercosis
Cysticercosis
Biopsies from cases of cercarial dermatitis show spongiosis and a mixed dermal inflammatory infiltrate comprising lymphocytes, histiocytes, eosinophilic leukocytes, and neutrophils. Intraepidermal cercariae may rarely be seen, if fortuitously included in the specimen.2
Fine needle aspiration cytology is a rapid and useful means of confirming the parasitic etiology thereof in such cases.8 The diagnosis of subcutaneous cysticercosis should prompt further investigations to rule out concomitant neurocysticercosis. The latter is a major cause of epilepsy in developing countries.1,2
Clinical features
The adult pork tapeworm Taenia solium may be present in the small intestine of man (the definitive host). The intermediate host, the pig, ingests the eggs, which develop to the cysticercus stage in muscle and elsewhere and is then infective if improperly cooked and eaten by humans. If humans ingest eggs, however, they can become the host for the cysticercus stage; this occurs most commonly in skin, subcutaneous tissue, skeletal muscle, brain, and eye.1,2 Disseminated cysticercosis may also involve the spinal cord, orbital soft tissues, liver, spleen, and rarely, the heart.3,4 Cystercerci in the skin present as painless nodules up to 2 cm across (Fig. 18.404). The vast majority of patients present with solitary subcutaneous nodules. Some patients, however, may present with multiple subcutaneous lesions.5 Nodules may also occur in the oral cavity or breast in a small percentage of cases; mammary lesions may mimic breast carcinoma clinically.6,7 In patients who are known to have an underlying malignancy, the evolution of multiple subcutaneous nodules of cysticercosis may be mistaken for metastases.
Pathogenesis and histologic features The viable cysticercus compresses adjacent dermis without inflammation and the diagnosis can be made by identification of the scolex (Fig. 18.405). However, when the parasite begins to degenerate there is an infiltration of neutrophils, histiocytes, and eosinophils, which becomes more granulomatous, with giant cells, fibrosis, and eventual calcification.
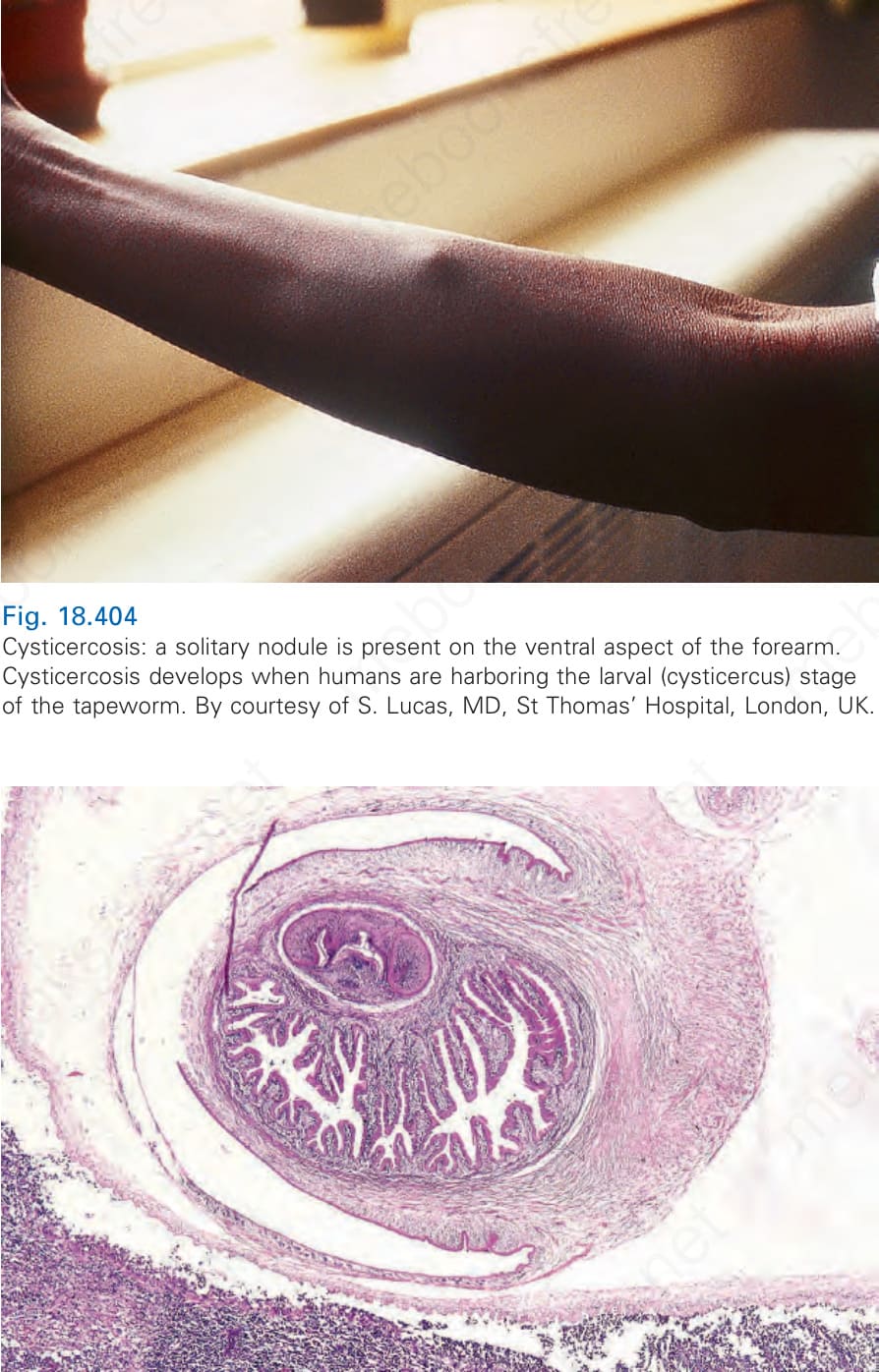
Fig. 18.404 Cysticercosis: a solitary nodule is present on the ventral aspect of the forearm. Cysticercosis develops when humans are harboring the larval (cysticercus) stage of the tapeworm. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.
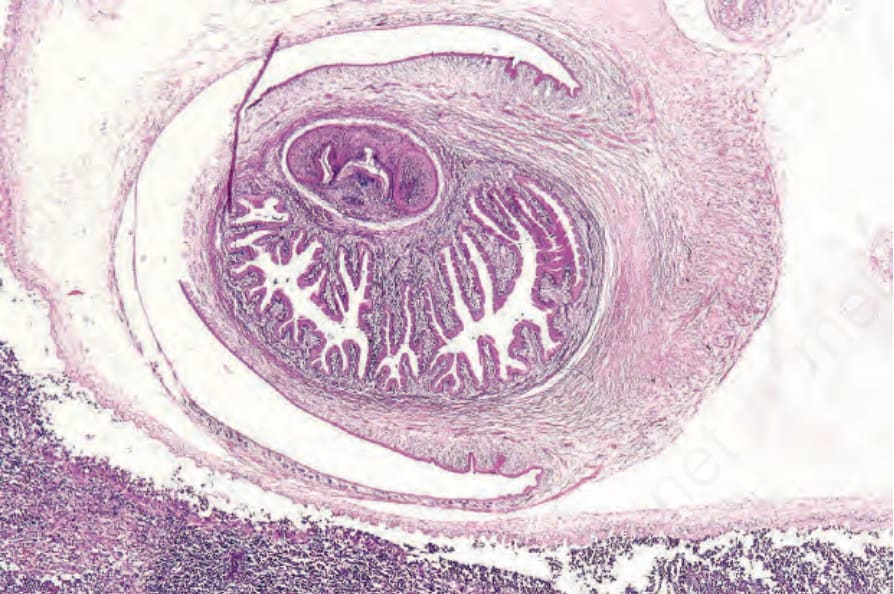
Fig. 18-405 (caption embedded in image / 圖說烘焙於圖內)